Childhood maltreatment and its associations with trauma-related psychopathology: disentangling two classification approaches

Introduction
One in four children experiences childhood maltreatment (CM)1, defined by the World Health Organization (WHO) as “all forms of physical and emotional ill-treatment, sexual abuse, neglect, and exploitation that results in actual or potential harm to the child’s health, development or dignity”2,3. CM significantly increases the risk of developing mental health disorders later in life, including post-traumatic stress disorder (PTSD), depression, and anxiety4,5,6,7. However, it remains less clear which CM experiences contribute most to different psychopathologies8,9. One potential factor worth exploring is the classification of CM experiences, as different classification approaches have been used in the field.
To date, two common approaches exist8,10,11. One approach characterizes CM based on the nature of maltreatment – abuse and neglect. Childhood abuse is defined as the presence of threatening input, namely, physical, emotional, or sexual, while childhood neglect is defined as the deprivation of key conditions, which could be either emotional (e.g., lack of emotional support) or physical (e.g., poor hygiene/malnutrition)12. This approach aligns with a developmental perspective of psychopathology arguing that threat and deprivation have distinct impacts on neurobiological development and psychopathology10,11,13. Previous studies using this approach revealed varying associations between childhood abuse and neglect sub-types and depression. Emotional abuse and emotional neglect consistently showed the strongest associations14, while separate studies indicated that individuals who experienced sexual abuse were more susceptible to depression and anxiety compared to other abuse and neglect subtypes15.
Another common classification approach for CM is the dimensional approach which categorizes the same five features of CM across three dimensions of maltreatment/human functioning: emotional (encompassing emotional abuse and neglect), physical (including physical abuse and neglect), or sexual (sexual abuse). Initial intriguing findings using this approach suggest that emotional16,17and sexual CM have a more pronounced impact on predicting symptoms of PTSD and depression, or general psychopathology including depression and anxiety, compared to physical CM. Yes, despite extensive research on CM and trauma-related psychopathology, a study exploring both CM approaches in relation to three trauma-related psychopathologies is absent.
Addressing the above-noted gap in knowledge, the aim of the current study is to utilize both CM classifications (i.e., abuse/neglect, dimensional approach) within a single cohort and to examine how each is linked to symptoms of PTSD, depression, and anxiety, using ordinary least squares regression analyses. We hypothesized that both the abuse/neglect and the dimensional approach classifications would be associated with these symptoms. Within the dimensional approach, and consistent with prior findings17, we hypothesized that emotional and sexual CM would be more strongly linked to PTSD, depression, and anxiety symptoms compared to physical CM. Finally, we hypothesized that the dimensional CM approach would be more effective and informative in predicting different symptoms compared to the abuse/neglect approach. On an exploratory level, and although mixed findings exist, we predicted that emotional abuse would exhibit the most robust association with depression, and sexual abuse would be most strongly linked to PTSD and anxiety. We did not have clear hypotheses about the associations between other specific subtypes of CM and each of these symptoms.
Results
Sample Clinical Characteristics
We recruited 685 individuals, 43 (6.2%) of whom were excluded for failing the inherent validity tests or had missing data, yielding a final sample of 642 individuals who completed all assessments (Mage = 36.8, SD = 11.3, 63.4% female; see Table 1 sample characteristics). Of the included participants, 43.1% met the cut-off score for PTSD (PC-PTSD ≥ 3). A total of 24.5% met the cut-off for mild depression (PHQ-9 ≥ 5 and ≤9), 22% moderate depression (PHQ-9 ≥ 10 and ≤14), and 26.3% moderately severe or more severe depression (PHQ-9 ≥ 15). A total of 31.5% met the cut-off for mild general anxiety (GAD-7 ≥ 5 and ≤9) and 40.2% met the cut-off for moderate-severe or more severe anxiety (GAD-7 ≥ 10).
As per the inclusion criteria, all participants experienced at least one type of CM, including Physical abuse (86.9%), Emotional abuse (90.7%), Sexual abuse (41.3%), Physical neglect (36.4%), and Emotional neglect (79.3%). As might be expected, we observed a significant level of co-occurrence among CM types across both CM classifications. Specifically, 535 participants had both abuse and neglect, and 107 (16.7%) participants reported experiencing abuse without neglect. Only 6 (0.9%) participants reported experiencing neglect (either physically or emotionally) but not abuse. As for the dimensional CM approach, 233 participants reported experiencing all three dimensions – sexual, physical, and emotional CM. A total of 564 participants experienced at least two CM dimensions across emotional/physical/sexual.
ANOVA tests
Model 1: Two-category dichotomous (abuse vs. neglect) approach.
Zero-order correlations between the variables can be found in Supplementary Table 1.
Table 2 summarizes the ANOVA results for abuse and neglect, and the dimensional CM approach. Significant main effects of abuse and neglect emerged for all three disorders. Abuse had the largest effect size among the main effects for PTSD, depression, and anxiety, as compared to neglect. No significant interaction effects were observed between abuse and neglect on PTSD, depression, and anxiety symptoms.
Model 2: three-category dimensional approach (Physical vs. Sexual vs. Emotional).
Significant main effects of physical and sexual CM emerged for PTSD but not for emotional CM. Significant main effects also emerged for emotional and sexual CM on depression and anxiety, but not for physical CM. Sexual CM had the largest effect size among the main effects for PTSD, depression, and anxiety. No significant interaction effects were observed among emotional, physical, and sexual CM on PTSD, depression, and anxiety symptoms.
Comparing the two CM classification approaches
We conducted OLS regression analyses to examine the effects of the two-category dichotomous (abuse vs. neglect) approach with the three-category dimensional approach (physical, emotional, and sexual) on all three symptom types. Table 3 summarizes the model fit indices (AIC and BIC) and R2 results for the OLS regression analyses comparing the two models. These results indicate that the Dimensional CM Approach outperformed the abuse/neglect classification in predicting all three symptoms. Specifically, the Dimensional CM Approach demonstrated higher R-squared values and lower AIC and BIC scores compared to the Abuse and Neglect classification model. This suggests that the Dimensional CM Approach may be more informative when examining the links between different CM experiences and symptoms of PTSD, depression, and anxiety.
In addition, SEM was employed to explore CM effects on PTSD, depression, and anxiety, comparing the two CM classification methods, while controlling for age, gender, ethnicity, race, social economics status, and prior treatment. Supplementary Table 2 presents the SEM model fit results, showcasing the comparison between the two classification approaches. As can be seen, the SEM analysis suggests that overall, the dimensional CM approach is more informative than the dichotomous abuse/neglect approach when predicting these symptoms.
Exploratory analyses– five categories of CM
We conducted OLS analyses to examine the effects of various CM experiences on symptoms of PTSD, depression, and anxiety (see Supplementary Table 3). When predicting PTSD using ‘Physical Abuse’, ‘Emotional Abuse’, ‘Sexual Abuse’, ‘Emotional Neglect’, and ‘Physical Neglect’, approximately 14.85% of the variability is explained by the included predictors and their interactions. The emotional neglect and sexual abuse were the top features predicting these symptoms (see Fig. 1). For depression, approximately 10.56% of the variability is explained by the included predictors and their interactions. The physical neglect and emotional abuse were the top features that predicted these symptoms (see Fig. 2). When predicting anxiety, approximately 9.49% of the variability is explained by the included predictors and their interactions. The emotional abuse and sexual abuse were the top features that predicted anxiety symptoms (Fig. 3).

Each bar represents the absolute value of the coefficient for the corresponding predictor variable, indicating the magnitude of its association with PTSD symptoms. The features are sorted by the absolute size of their coefficients, with larger bars indicating a stronger relationship with the dependent variable.
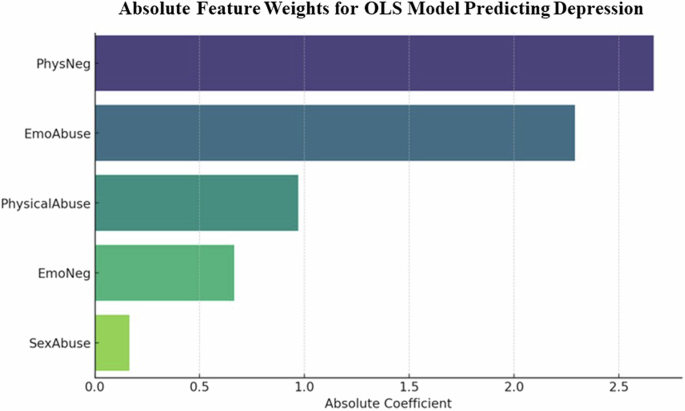
Each bar represents the absolute value of the coefficient for the corresponding predictor variable, indicating the magnitude of its association with depression symptoms. The features are sorted by the absolute size of their coefficients, with larger bars indicating a stronger relationship with the dependent variable.
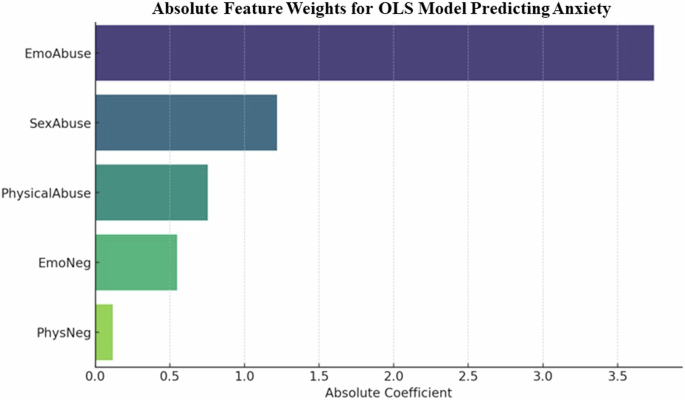
Each bar represents the absolute value of the coefficient for the corresponding predictor variable, indicating the magnitude of its association with anxiety symptoms. The features are sorted by the absolute size of their coefficients, with larger bars indicating a stronger relationship with the dependent variable.
Discussion
The aim of this study was to assess how specific classification features are linked to different psychopathologies across two common classification systems and which classification demonstrates the most pronounced links to different psychopathologies. Across both classifications, the same five CM experiences were included: Sexual abuse, Physical abuse, Emotional abuse, Physical neglect, and Emotional neglect. In the first approach, which classifies CM experiences as abuse or neglect, both were linked to all types of symptoms. Specifically, PTSD was associated with sexual abuse and emotional neglect; depression was associated with emotional abuse and physical neglect; and anxiety was associated with sexual abuse and emotional abuse. None of these symptoms were associated with physical abuse. These findings suggest the unique role of emotional neglect in understanding PTSD, and physical neglect in assessing depression symptoms. In the second classification, the Dimensional CM Approach, which classifies CM experiences as dimensional (sexual, physical, emotional), all symptom types were associated with sexual CM, depression and anxiety symptoms were exclusively associated with emotional CM, and only PTSD was linked to physical CM.
Our findings using the abuse/neglect approach support the conclusion of Humphreys et al.14 that emotional abuse is particularly associated with depression. Interestingly, contrary to their finding, we did not observe a strong association between emotional neglect and depression; instead, we found a notable link with physical neglect. The discrepancy in these findings may be attributed to variations in sample characteristics or assessment methods and more studies, especially longitudinal ones, are needed to clarify and validate the distinct effects of childhood physical versus emotional neglect on depression. Furthermore, our results are in line with previous studies suggesting that individuals who have experienced childhood sexual abuse could be more susceptible to anxiety and PTSD18 compared to those experiencing other forms of abuse and neglect.
Our findings using the Dimensional CM Approach are partially congruent with previous research17 suggesting that PTSD and depression symptoms are more strongly linked to sexual CM, as compared to physical CM. In contrast to their findings, in our study, only depression, but not PTSD, was linked to emotional CM. Our findings further extend these results by suggesting a link between anxiety and emotional and sexual CM. Moreover, similar to the findings by Iffland et al.16, emotional CM, but not physical CM, was linked to symptoms of depression and anxiety.
Analyzing the data using both the abuse/neglect and dimensional CM classifications revealed distinct associations between CM experiences and psychopathologies. For instance, the abuse/neglect approach did not reveal significant links between depression and sexual abuse, while the dimensional CM approach, utilizing the exact same variables, showed significant associations (with sexual CM being the top feature for depression). These findings emphasize that researchers’ choices in defining and analyzing CM, based on either classification system, can significantly impact the observed associations with psychopathologies, with clinical implications. Careful consideration of the classification framework is crucial for identifying relationships between specific CM experiences and psychopathological outcomes. Researchers and clinicians should be aware of the potential variability introduced by the chosen classifications systems, affecting the interpretation of study results and guiding targeted interventions. This understanding, and the somewhat contradictory findings observed in our study, motivated our desire to compare the utility of these two CM classifications in predicting these outcomes.
Compared to the abuse/neglect classification, the Dimensional CM Approach emerged as a more informative classification for predicting all three types of symptoms. That is, focusing on the dimension of maltreatment might be more informative/useful when trying to understand symptoms of PTSD, depression, and anxiety, as compared to the traditional dichotomous abuse/neglect approach. Our findings suggest the need to consider CM assessment tools that incorporate a dimensional approach. In addition, the results suggest the potential for tailored therapeutic approaches by identifying and addressing specific symptomatology associated with emotional, sexual, or physical maltreatment. For example, interventions for individuals who experienced emotional CM might focus more on addressing issues related to depression and anxiety, while those who experienced physical CM might require tailored support for PTSD symptoms. However, the frequent co-occurrence of these CM experiences makes it difficult to identify the unique effects of CM experiences19 and this should be taken into account when interpreting the findings.
While the increase in R² from the dichotomous abuse vs. neglect classification approach to the dimensional CM approach was modest (ranging from 0.1% to 0.7%), this difference could still be clinically and practically meaningful. Transitioning from a dichotomous to a more granular three-category approach of CM allows for a more detailed characterization of CM types and a better understanding of its potential associated effects. Each dimension of CM (physical, sexual, and emotional) may be associated with different mental health outcomes (e.g., PTSD symptom severity). By distinguishing these types, this dimensional approach potentially increases the sensitivity to detect specific effects of different CM types on various clinical outcomes.
This study has several limitations. One limitation is that single items were used to assess each type of maltreatment, without properly assessing the severity of CM. Future studies are needed for additional and more nuanced assessments to provide a comprehensive understanding of the complex nature of CM and its impacts. Relatedly, given the considerable overlap in reported types of CM both in the literature and our study, the interpretations of the findings are somewhat limited. However, since this overlap simply reflects the reality of CM survivors who often face several CM experiences, this study suggests that classifying these experiences based on a dimensional approach might be more informative when trying to assess/predict potential trauma-related mental health outcomes. Second, we used self-report measures. Moreover, although our models show a statistically significant increase in R², the small magnitude of this increase necessitates a cautious interpretation, especially when considering the translation of these findings into clinical settings. In addition, we used brief screening tools for PTSD, depression, and anxiety. While brief self-report measures are widely used and provide insights into individuals’ behavior20, future studies may wish to include performance-based paradigms and neurobiological measures, as well as clinical diagnostic interviews to complement and validate these findings. Third, the data quality of online panels has been criticized recently for representativeness of samples and their susceptibility to response bias21. However, Chmielewski & Kucker22 suggest that these effects can be mitigated by using response validity indicators and screening the data, which we implemented via attention checks. Still, the potential for self-reporting bias when using these platforms, especially for sensitive questions such as CM, should be acknowledged. Future research should employ a variety of platforms and more rigorous inclusion criteria to further validate our findings. Fourth, while the current demographic allows generalization of the findings to more segments of society (in line with the RDoC framework23), future examinations may test the relationships between CM and these symptoms in clinically diagnosed individuals with elevated symptom levels. Such studies may assess whether and how specific symptom clusters are linked to different CM experiences. Finally, the cross-sectional design of this study precludes making causal inferences about the relationships between CM and symptoms. Therefore, future investigations should clarify these relationships over time by incorporating longitudinal research. Future studies could also benefit from comparing gender effects in understanding the link between diverse CM experiences and psephology and assessing the mediating role of the timing of these experiences (e.g., early versus late childhood) and their frequency (single or recurrent).
In summary, our findings refine our understanding of the intricate relationships between CM experiences and symptoms of depression, PTSD, and anxiety. Comparing two common classifications—abuse versus neglect and the Dimensional CM Approach—we found that both abuse and neglect predict various symptoms, but with limited predictive significance. Notably, the Dimensional CM Approach demonstrated superior efficiency in capturing the contributions of different CM dimensions to PTSD, depression, and anxiety symptoms. These results underscore the importance of a dimensional approach in understanding the impact of maltreatment experiences on mental health. Despite study limitations, our findings suggest the potential for tailored therapeutic approaches by identifying and addressing specific symptomatology associated with emotional, sexual, or physical maltreatment. Ultimately, this research lays the groundwork for developing targeted early interventions and treatment strategies for individuals affected by depression, PTSD, and anxiety in CM survivors.
Methods
Participants
Participants were recruited through Cloud Research and Amazon Mechanical Turk (MTurk) from May to July 2023. These crowdsourcing platforms are used often in psychology and psychiatry research with evidence of validity across tasks24,25. Previous studies support the use of MTurk for researching sensitive topics, such as childhood adversity and maltreatment26,27. To verify the validity of the study’s results, we excluded respondents who failed more than one of our three attention-checks (e.g., “In the following question, please choose ‘I agree’”) or were classified as bots using CAPTCHA. Participants were all English-speaking US residents, aged 18–80, who reported at least one childhood adversity (see below). Participants were compensated $3 for study participation. The study was approved by the New York State Psychiatric Institute Institutional Review Board (#8453). Prior to the study, participants reviewed an informed consent form. Those who agreed to participate completed the study procedures via Qualtrics.com, a secure, online data collection platform.
Measures
Instruments included measures for childhood maltreatment, PTSD, depression, anxiety, and sociodemographic variables. Childhood Maltreatment experiences included physical, emotional, or sexual abuse, or physical and emotional neglect up to age 18. Specifically, participants were asked: While you were growing up, during your first 18 years of life, did you experience any of the following? (Select all that apply.) (1) On one or more occasion/s, a family or household member was physically aggressive with either you or another family member (i.e., physical abuse); (2) a family member swore at you, criticized you, humiliated you, or threatened you (i.e., emotional abuse); (3) You experienced an unwanted or inappropriate sexual experience/s (i.e., sexual abuse); (4) On one or more occasion/s, you didn’t have enough to eat, had to wear dirty clothes, had no one to take care of you, or had caregivers who were too drunk or high to take care of you (i.e., physical neglect); (5) You felt unloved or unsupported by your family, or felt like family members were not concerned about, or supportive of, each other (i.e., emotional neglect).
We assessed clinical symptoms of PTSD using the Primary Care PTSD Screen for DSM-5 (PC-PTSD-5)28,29. We adjusted PC-PTSD-5 items to focus on CM-related events (e.g., “In the past month, have you felt guilty or unable to stop blaming yourself for the childhood-abuse related events?”). Higher scores indicating greater self-reported symptom severity. Internal consistency in the current sample α = 0.74 for PTSD.
Depression was assessed using the Patient Health Questionnaire-9 (PHQ-9)30, a brief instrument assessing nine depressive symptoms experienced over the past two weeks. Responses are scored from 0 = “not at all” to 3 = “nearly every day”. Symptom severity is indicated by the sum of all item scores. The psychometric properties of this measure proved to be adequate with a robust factor structure and good internal consistency31. Internal consistency in the current study was α = .90.
We used the Generalized Anxiety Disorder-7 (GAD-732) to assess seven generalized anxiety symptoms during the past two weeks, each rated on a scale ranging from 0 (“not at all”) to 3 (“nearly every day”), with an overall score range of 0–21. Higher scores indicate greater self-reported anxiety. Internal consistency in the current study a = 0.92.
Sociodemographic variables, including age, gender, race, ethnicity, socio-economic status, and prior treatment were assessed using a brief self-report questionnaire.
Procedure
The study was pre-registered on Clinical Trials in April 2023 (NCT05818228) and contains new unpublished data which was collected as part of a larger interventional study assessing the effectiveness of an online intervention in reducing self-stigma among CM survivors29. The study was described as a research project on “self-stigma among childhood maltreatment survivors”. Consented participants first completed a demographic questionnaire, followed by the above-described measures.
Data analysis
Data analysis was performed using Python with packages pandas, sklearn, and scipy33,34,35. For the structural equation models (SEM) exploratory analyses we utilized the lavaan package in R and employed the Maximum Likelihood Estimation (MLE) method under robust conditions. SEM accommodates complex associations, latent variables, and multiple interrelated dependent variables, adjusting for covariates. We used G*Power software36 to calculate the required sample size based on our previous study29.
To test our hypotheses as part of the main analysis, we first conducted a separate Analysis of Variance (ANOVA) test for each of the two different CM classifications (i.e., abuse/neglect, and dimensional approach) and the three symptoms: PTSD, depression, and anxiety. These analyses aimed to examine the main and interaction effects of CM classification on PTSD, depression, and anxiety symptoms. For example, a two-way ANOVA assessed the impact of abuse (a categorical variable with four levels: sexual, emotional, physical, and total abuse) and neglect (a categorical variable with three levels: emotional neglect, physical neglect, and total neglect) on PTSD symptoms. Same analyses were conducted for depression and anxiety as dependent variables. The p values were corrected using Bonferroni correction.
To interrogate the links between various CM experiences and symptoms of PTSD, depression, and anxiety, we first conducted Ordinary Least Squares (OLS) regression analyses to examine the effects of the two-category dichotomous (abuse vs. neglect) approach with the three-category dimensional approach (physical, emotional, sexual) on all three symptom types. R-squared (R²), Akaike Information Criterion (AIC), and Bayesian Information Criterion (BIC) were reported to measure the goodness of fit of these models.
In addition, SEM was employed to explore CM effects on PTSD, depression, and anxiety, comparing the two CM classification methods, while controlling for age, gender, ethnicity, race, social economics status, and prior treatment. Model fit indices such as Comparative Fit Index (CFI), Tucker-Lewis Index (TLI), Standardized Root Mean Square Residual (SRMR), and Root Mean Square Error of Approximation (RMSEA) were calculated.
For exploratory analyses, we assessed the superiority of each CM classification in its associations with specific disorder outcomes, we re-ran the OLS regression analyses. Each disorder (i.e., PTSD, depression, or anxiety symptoms) served as the dependent variable, with predictors including using ‘Physical Abuse’, ‘Emotional Abuse’, ‘Sexual Abuse’, ‘Emotional Neglect’, and ‘Physical Neglect’. R², AIC, and BIC were used as quantitative measures to evaluate the goodness of fit and compare the two regression models.


Responses