Utilization of plant-based foods for effective prevention of chronic diseases: a longitudinal cohort study

Introduction
Chronic diseases, particularly cardiovascular diseases (CVDs) and diabetes, pose a significant global health burden1,2. CVDs remain the leading cause of mortality worldwide, while diabetes contributes substantially to premature deaths3,4. The high prevalence and impact of these conditions highlight the urgent need for effective prevention and management strategies.
Improving cardiovascular and metabolic health worldwide requires tailored strategies, as different populations have varying susceptibilities to risk factors influenced by their lifestyle choices, particularly diet. A multicenter trial in Spain with 7447 high-risk CVDs participants found that those on a Mediterranean diet supplemented with olive oil or nuts had fewer cardiovascular events than those on a low-fat diet5. A systematic review of 28 meta-analyses confirmed that a higher intake of fruits, vegetables, nuts, seeds, and whole grains reduces CVDs risk, while processed meats and sugary drinks increase it6,7. Furthermore, several meta-analyses have shown that a healthy plant-based diet, which is characterized by a high intake of nutrient-rich plant-based foods and a low intake of refined carbohydrates and animal products, is linked to a decreased risk of CVDs mortality and all-cause mortality8,9,10. A cohort study from the UK Biobank involving 126,394 participants found that such diets are associated with reduced mortality and chronic disease risk11. As plant-based diets gain popularity globally12,13, their health benefits become increasingly significant, especially for chronic diseases.
However, current research based on longitudinal cohort studies examining the relationship between plant-based foods and chronic disease risk often relies on two implied assumptions. The first assumption posits that dietary intake, measured at baseline, remains constant over time14. This perspective neglects the natural fluctuations in eating habits during long-term follow-up periods, potentially resulting in inaccurate assessments of the true impact of diet on health outcomes. Furthermore, accurately assessing these effects in longitudinal cohort studies is further complicated by the dynamic nature of food intake and the influence of time-varying confounding factors15,16. The second assumption is that researchers often assume a linear relationship between food intake and disease risk. To simplify the analysis, continuous food variables are typically categorized into groups based on medians or quartiles17, which can create the impression that a higher intake of certain foods is always beneficial for health. In reality, the mechanisms linking plant-based foods to chronic disease risk are more complex and may not follow a straightforward linear pattern. Therefore, it is essential to adopt more nuanced approaches that offer clearer guidance on optimal dietary intake levels.
Furthermore, much of the current research focuses on individual chronic diseases, despite the frequent co-occurrence of multiple conditions. Understanding how plant-based foods influence the risk of several chronic diseases simultaneously is crucial for developing comprehensive dietary recommendations that address the overall burden of chronic illness. Additionally, gender-specific dietary preferences and differences in chronic disease incidence are well-documented18,19,20,21, yet many studies neglect these differences, resulting in generalized recommendations that may not be equally applicable to both men and women. Analyzing the effects of plant-based diets separately for men and women could provide more targeted dietary guidance, tailored to the specific health needs of each gender.
Therefore, our study is based on a longitudinal cohort study of the China Health and Nutrition Survey (CHNS) data from 2004 to 2015. After using residual balancing weights (RBW) to effectively control for time-varying confounding factors22, the restricted cubic spline (RCS) model23 was further used to investigate the average dose-response relationship between the consumption of plant-based foods and the incidence of four chronic diseases. Additionally, we explore gender disparities to personalize the utilization of plant-based foods to prevent chronic diseases effectively.
Results
Baseline characteristics of the study populations
Table 1 shows the baseline characteristics of participants in our study. Of the participants, 46.7% were men, with a mean age of 45 years. Seventy-three percent lived in rural areas, 28.1% were current smokers, and 84.4% reported drinking alcohol. Women were more likely than men to have lower educational attainment, lower incomes, higher BMI, lower energy intake, and more activity. Additionally, significant gender differences were found in plant-based food intake. Men had higher intakes of refined grains, vegetables, tubers, legumes, and nuts and seeds, while women consumed more fruits.
Incidence of chronic diseases over 12 years follow-up
In the baseline year (2004), all participants were free from chronic conditions including hypertension, stroke, myocardial infarction, and diabetes. During the four follow-up periods from 2006 to 2015, 1237 new cases of hypertension were recorded in men and 1221 in women. Among men, the highest incidence was in 2006 (14.3%), followed by declines in subsequent follow-ups (13.9% in 2009 and 9.5% in 2011), with a slight increase in 2015 (13.2%). In women, incidence peaked in 2009 (11.9%), then decreased (7.3% in 2011), with a small rise again in 2015 (11.1%).
Regarding stroke, there were 62 new cases among men and 30 in women. Men’s highest incidence was in 2009 (0.7%) and lowest in 2015 (0.3%). Women’s lowest incidence was in 2006 (0.1%), with gradual increases over time. New myocardial infarction cases totaled 41 in men and 37 in women, peaking in men in 2006 (0.4%) and showing a downward trend thereafter, while women’s lowest incidence was in 2006 (0.2%), increasing over time. Diabetes cases totaled 84 in men and 81 in women; men’s highest incidence was in 2009 (1.2%), while women’s was lowest in 2006 (0.5%) and rose in subsequent follow-ups. Figure 1 illustrates the distribution and cumulative incidence of these chronic diseases by gender over the study period, consistently showing higher incidence rates in men than in women across all conditions.

Data represent the results from 6317 participants in CHNS.
Time trends of plant-based foods over four follow-up waves
Except for legumes in men (P for trend = 0.1916), the average consumption of other plant-based foods showed significant time-varying trends (all P for trend <0.0010) (Fig. 2). Refined grains, vegetables, and tubers exhibited overall declining trends. Among these, the decline in refined grains was relatively modest (7% in men and 9% in women), while the decrease in tuber consumption was more substantial (80% in men and 79% in women), followed by vegetables (27% in men and 28% in women). In contrast, the intake of fruits, fungi and algae, and nuts and seeds showed an overall upward trend. The largest increase was seen in fruits consumption (279% in men and 249% in women), while the intake of nuts and seeds, as well as fungi and algae, more than doubled (nuts and seeds: 118% in men and 161% in women; fungi and algae: 109% in men and 110% in women). Whole grains and legumes exhibited fluctuations, but the changes were relatively minor, with the maximum fluctuation not exceeding 50% (<48% for whole grains and <20% for legumes). Additionally, except for tubers (interaction P = 0.0081), there were no significant gender differences in these time trends (interaction P > 0.0500). However, at each time point, significant gender differences were observed in the consumption of whole grains, vegetables, and legumes (P < 0.0500). While the intake of tubers, fruits, and nuts and seeds appeared gender difference only at the baseline or in the earlier measurement periods (P < 0.0500).
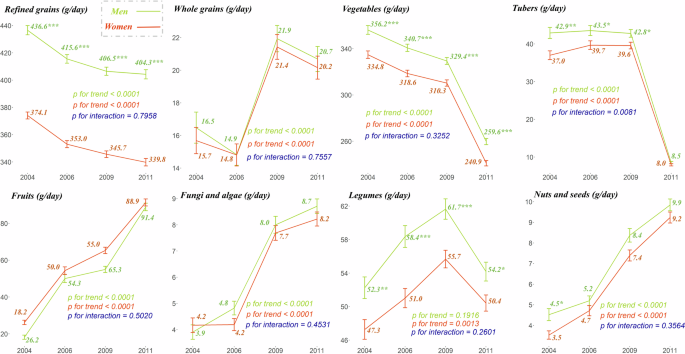
Error bars indicate standard error. The P values were calculated using the generalized estimating equations. The P for trend (<0.0500) indicates the significant main effect of time. The P for interaction (<0.0500) indicates the significance of interaction effects between gender groups and time. The asterisks indicate the comparison of average food intake between gender groups at each time point. * indicates P < 0.0500. ** indicates P < 0.0100. *** indicates P < 0.0010. Data represent the results from 6317 participants in CHNS.
Identification of time-varying confounders
The covariates, including education level, annual income, sleep duration, BMI, physical activity level, smoking, drinking status, and energy intake, displayed dynamic trends over time, all exhibiting P for trend <0.0001 (see Supplementary Table S1).
Average dose-response associations of plant-based foods to chronic disease risk
The average intake of plant-based foods and their dose-response relationships with the risks of four chronic diseases predominantly exhibited non-linear patterns (Fig. 3). Specifically, the average intake of whole grains and vegetables demonstrated curvilinear inverse relationships with the risks of these diseases. Similarly, the average intake of fruits, fungi and algae, and nuts and seeds also showed negative correlations with the risks of these four chronic diseases. However, an exception was observed as the average intake of fungi and algae among men showed a parabolic relationship with the risk of hypertension. This indicates that the intake of fungi and algae should be maintained within a moderate range (10–33 g/day). A similar finding was observed in women, where fruit intake within a range of 188–295 g/day is associated with hypertension prevention. Additionally, higher consumption of nuts and seeds in men was linked to an increased risk of diabetes.
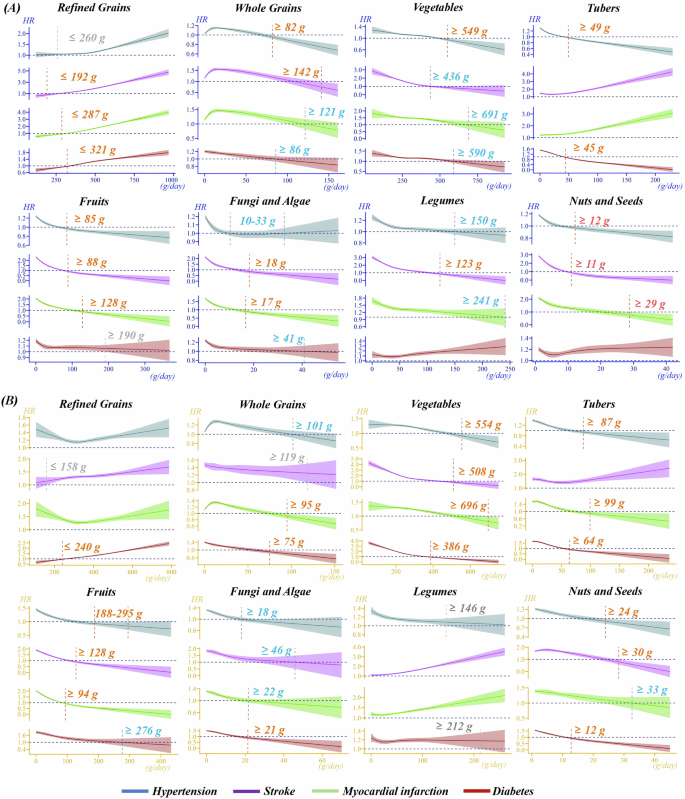
A Men, B Women. These relationships were estimated by RCS based on RBW. The cutoff value with red color, indicating HR < 1 and 95%CI not containing 1, signifies the prevention of chronic disease incidence within this scope. The blue intake range corresponds to HR < 1 but with a 95% CI that contains 1, while the gray intake range corresponds to HR > 1 but with a 95% CI that contains 1, suggesting that the risk of chronic disease incidence no longer increases within this range. Data represent the results from 6317 participants in CHNS.
In men, the average intake of refined grains showed curvilinear positive relationships with the risks of all four chronic diseases, meaning that greater intake correlates with higher risks. However, when consumption was below the recommended cutoff amount, it could be beneficial for preventing these diseases. For women, the same trend was observed only concerning stroke and diabetes, and regardless of the amount consumed, refined grains increased the risks of hypertension and myocardial infarction. Furthermore, the dose-response relationships for tubers and legumes showed inconsistencies in relation to different chronic diseases risks. The dose-response relationships for tubers and legumes exhibited inconsistencies between genders. Specifically, the average intake of tubers was associated with curvilinear inverse relationships concerning hypertension and diabetes, while showing curvilinear positive relationships with stroke risk. Notably, any level of tuber intake increased the risk of stroke, and the relationship with myocardial infarction varied between men and women. For legumes, the average intake presented curvilinear inverse relationships with hypertension, while the associations with stroke, myocardial infarction, and diabetes differed based on gender. Specific cutoff values and the corresponding HR and its 95%CI values were presented in Supplementary Table S2, and the results of the non-linear tests for the dose-response curves were detailed in Supplementary Table S3.
Figure 4 presents the plant-based food pyramid for different gender groups, based on the recommended intake cutoff values for various chronic diseases depicted in Fig. 3. Regardless of gender or type of chronic disease, sufficient intake of vegetables and whole grains was beneficial in preventing four chronic diseases simultaneously. Specifically, adequate vegetable consumption in women showed significant protective effects (HRs < 1, with 95% CIs not containing 1). Additionally, in men, sufficient intake of fruits, moderate consumption of refined grains, and a certain amount of fungi and algae were associated with a reduced risk of these chronic diseases. For women, sufficient intake of fungi and algae, as well as nuts and seeds, along with moderate fruit consumption, was linked to a lower risk of developing these four chronic diseases simultaneously.
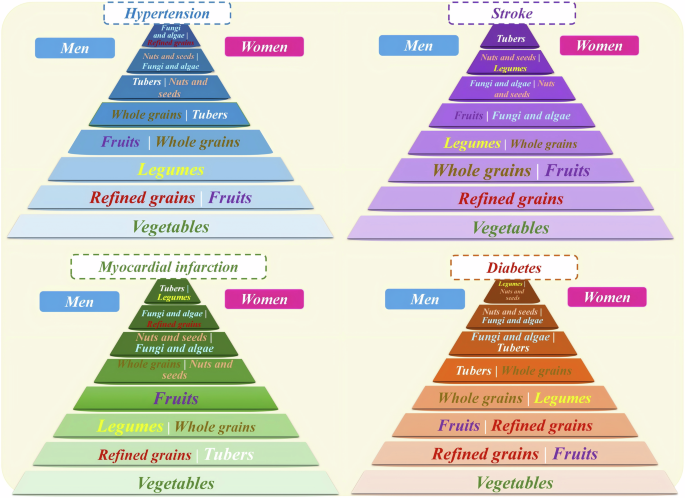
The position of the foods in the pyramid was determined by the size of the cutoff values. The plant-based foods with higher cutoff values were ranked at the bottom, and the plant-based foods with lower cutoff values were ranked at the top.
Moreover, the sensitivity analysis indicated strong overlap between the results from the dataset without imputed missing data and those with imputed data, with both displaying a consistent overall trend (Supplementary Fig. S1). Although there were some differences in the cutoff values, they were numerically close, further demonstrating the robustness of our findings. However, we did observe a few discrepancies. In the sensitivity analysis, the recommended fruit intake for preventing hypertension and diabetes in men was within a specific optimal range, rather than indicating “the more, the better.” Similarly, in women, the intake of fruits and fungi and algae also showed an optimal range for reducing the risk of diabetes and hypertension, rather than a continuously increasing benefit. Additionally, the sensitivity analysis revealed that in men, increased consumption of legumes (≥104 g/day) and nuts and seeds (≥14 g/day) was associated with no further increase in diabetes risk once intake reached certain levels. For women, a higher intake of refined grains (≥653 g/day and ≥626 g/day, respectively) did not lead to an increased risk of hypertension and myocardial infarction. However, specific cutoff values for these foods were not identified in Fig. 3. Notably, it was consistently observed that none of these foods showed significant protective effects in either the main analysis or the sensitivity analysis (HRs’ 95% CI included 1).
Figure 5 presents an overview summarizing the key findings of this study based on the results.
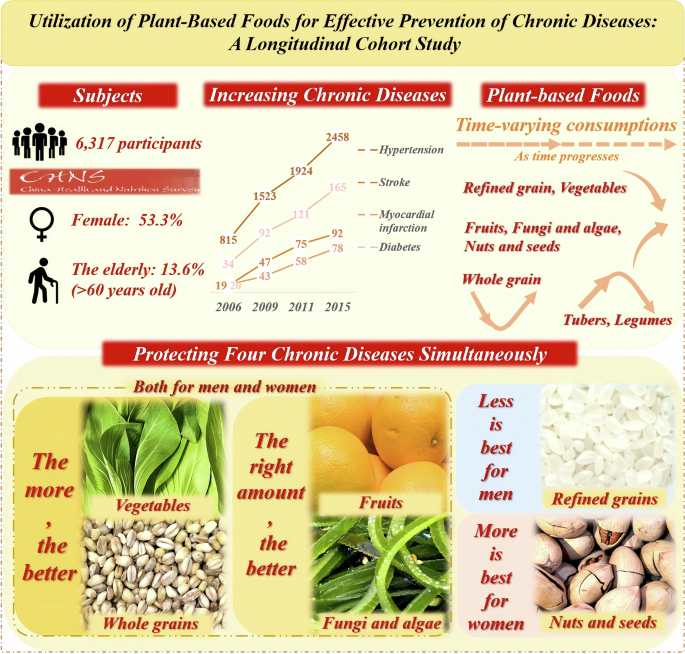
Overview of study subjects, the increasing prevalence of chronic diseases from 2006 to 2015, evolving plant-based foods consumption trends (arrows indicate the direction of change over time: downward for decrease, upward for increase, and mixed for fluctuations), and their combined roles in preventing four chronic diseases (colors emphasize gender-specific recommendations).
Discussion
The longitudinal study, based on the CHNS, demonstrated a gradual increase in the cumulative incidence of the four chronic diseases over the five survey periods. Furthermore, it revealed that the incidence of new chronic disease cases was consistently higher in men than in women. The mean intake of almost all plant foods demonstrated significant time-varying trends, yet the magnitude of change in intake of different plant foods differed between men and women. The findings indicated that a high intake of vegetables and whole grains, along with moderate amounts of fruits, fungi and algae, could reduce the simultaneous risk of these four chronic diseases. Additionally, men could benefit from moderate refined grain consumption, while women should increase their intake of nuts and seeds. Furthermore, additional covariates, including physical activity level, sleep duration, annual income, body mass index, energy intake, educational level, smoking and drinking status, demonstrated time-varying characteristics. Sun and colleagues conducted a systematic review of 94 cohort studies from the Western Pacific region and identified a shift towards healthier dietary intake patterns over the past three decades24. This suggests that dietary covariates associated with lifestyle behaviors are not fixed24. When both food intake and covariates are time-varying in nature, feedback between food exposure and covariates occurs, which is the current food intake is influenced by past covariates and also the level of covariates in the next cycle. For example, people who consumed more refined grains in the past tended to have higher BMI values or energy intake levels, but subjects with higher BMI values or energy intake levels may adjust grains later in the study to lower or maintain their own BMI levels or energy intake levels25,26. Another example is that lower fruit intake may be associated with lower levels of income or lower levels of education and that an increase in subjects’ income level or education level over time may in turn increase fruit intake27,28. Similar Feedback may also exist with vegetables and exercise levels29, nuts and seeds, and hours of sleep30. Such Feedback exists when Conventional approaches for controlling time-varying confounders such as stratification, regression correction, and propensity score matching have been proven ineffective in managing time-varying confounders. Therefore, we used the new method RBW capable of handling this Feedback in combination with RCS to estimate the mean dose-response relationship between plant-based foods and chronic disease risk.
Existing research has predominantly focused on comparing plant-based diets with other dietary patterns or categorizing them along a continuum of intake or dietary index to conclude that higher consumption of plant-based foods is more beneficial to health. For instance, a systematic review and meta-analysis of 20 clinical trials revealed that individuals at high cardiovascular risk experienced slight but significant improvements in cardiometabolic health indicators after adopting a vegan diet31. Similarly, several studies have demonstrated that vegetarian diets lead to more substantial improvements in blood pressure reduction, weight loss, and glycemic control compared to omnivorous diets32,33,34. Additionally, a study involving 11,825 Spanish participants found that adherence to the Healthy Plant-Based Diet Index was significantly associated with a reduced risk of CVDs mortality35. However, these studies often did not specifically quantify the intake of plant-based foods, potentially overlooking critical information. For example, our study found that to reduce the risk of hypertension in women, fruit intake should be within the range of 188–295 g/day, rather than excessively high. Furthermore, a prospective cohort analysis involving 135,335 individuals aged 35 to 70 years from seven regions and 18 countries demonstrated that a higher total intake of fruits, vegetables, and legumes (measured in servings) was significantly and inversely associated with major cardiovascular events and all-cause mortality36. While that study quantified intake by servings, our research provided more detailed information on the intake of specific plant-based foods, thereby enhancing the precision and quantitative depth of the findings.
Our study diverges from existing findings by revealing that the relationship between plant-based food intake and chronic disease risk is predominantly non-linear. This non-linear relationship varies across different food groups, diseases, and genders. Specifically, the average intake of whole grains and vegetables demonstrated curvilinear inverse relationships with the risk of developing four chronic diseases in both genders. Notably, high levels of whole grains intake exhibited protective effects against hypertension and stroke in men and myocardial infarction in women. However, for other diseases, no significant protective effect was observed, but exceeding a certain level of whole grains intake did not increase disease risk. These findings align with previous research indicating that increased whole grains consumption reduces the risk of CVDs and diabetes37,38. The potential mechanisms underlying these protective effects include the high dietary fiber content in whole grain foods, which promotes satiety, delays gastric emptying, prolongs nutrient absorption, and modulates postprandial insulin and glucose responses39. These factors contribute to weight loss and the long-term maintenance of a healthy body weight, thereby reducing disease risk. Additionally, the digestive and viscosity properties of dietary fiber, along with its components such as arabinoxylan, inulin, pectin, bran, and resistant starch, play a significant role in improving human health40.
When vegetable intake is maintained at a high level, significant protective effects are observed against hypertension in men and all four chronic diseases in girls, without increasing the risk of stroke, myocardial infarction, and diabetes in men. Established studies corroborate these findings. For instance, Aune et al. synthesized data from 95 studies, revealing a negative association between fruits and vegetables consumption of up to 800 g per day and CVDs41. Similarly, Zhan et al. reported a significant reduction in CVDs risk when comparing the highest to the lowest levels of vegetables intake42. The protective benefits of vegetables may be attributed to their rich content of dietary bioactives, particularly polyphenols and carotenoids43. While carotenoids are often regarded as simple biomarkers of vegetable intake, they possess significant anti-inflammatory and antioxidant properties43. Additionally, vegetables are abundant in dietary fiber, which is known for its cholesterol-lowering effects. These mechanisms collectively provide robust support for the role of high vegetable intake in reducing the risk of chronic diseases.
The average intake of fruits, fungi and algae, nuts and seeds also showed similar negative associations with the risk of the four chronic diseases. This finding aligns with existing studies, for instance, Lukas et al. found that a daily intake of 100 g of fruit significantly reduces the risk of hypertension37. Additionally, a meta-analysis of 123 studies demonstrated that the highest compared to the lowest intake of fruits significantly decreases the risk of stroke7. Similarly, myocardial infarction44 and diabetes45 also benefited. The potential biological mechanisms underlying these benefits include increased antioxidant capacity46, anti-inflammatory effects47, prevention of platelet aggregation, and reduction of vascular tone48. Fungi and algae, rich in key nutrients and various health-promoting compounds, also show significant benefits in chronic diseases49,50. These foods are an important source of phenolic compounds, flavonoids, and polysaccharides50, which exhibit antioxidant, antimicrobial, and anti-inflammatory properties by scavenging and neutralizing free radicals. Consequently, they may combat many common diseases, including atherosclerosis, diabetes, and CVDs51,52.
Similarly, studies have demonstrated that a daily intake of 28 grams of nuts and seeds is associated with a 21% reduction in the risk of CVDs compared to no intake of nuts and seeds53. Nuts and seeds are a valuable source of protein, and it has been established that vegetarians consume plant proteins as a substitute for animal proteins to help mitigate their risk of developing chronic diseases such as diabetes and heart disease54. However, our findings also indicated a parabolic relationship between the average intake of fungi and algae and the risk of developing hypertension in men, as well as a parabolic relationship between the intake of fruits and the prevention of hypertension in women. This suggests that a higher intake of fungi and algae in men and fruits in women is not necessarily more beneficial in terms of hypertension. The existing studies, which are based on linear assumptions, for example, those of Borgi55, Kim et al.56, can only conclude that a higher intake is beneficial. The mechanism may be that fruits are high in fructose and that excessive intake may lead to higher blood uric acid levels57. It has been demonstrated that elevated blood uric acid levels constitute a risk factor for hypertension58. Furthermore, although fruits are typically rich in potassium, excessive fruits intake without an equivalent increase in sodium intake and an imbalance in the potassium-sodium ratio may impact blood pressure regulation59. Furthermore, although mycorrhizal foods are rich in a variety of bioactive compounds, the parabolic pattern of mycorrhiza and the risk of hypertension in men indicates the necessity for greater attention to be paid to dietary intake. Consequently, further in-depth studies are required in the future to determine the optimal level of intake.
Existing studies have concluded that refined grains are unhealthy and that they should be replaced completely with whole grains as much as possible26. Our study confirms these findings, showing a positive association between refined grain consumption and chronic disease incidence. However, our research also reveals nuanced gender-specific effects. For men, a low intake of refined grains was associated with a reduced risk of chronic diseases, or at least a stabilization of risk levels. In women, while a low intake of refined grains reduced the risk of diabetes, it did not offer protection against other chronic diseases. Nonetheless, the risk did not increase below a certain consumption threshold. Therefore, our study suggests maintaining a low intake of refined grains rather than complete elimination. It is important to note that entirely replacing refined grains with whole grains, without considering fortified grain products, could result in nutritional deficiencies60. The consumption of fortified refined grain foods can help mitigate these deficiencies61.
Given that current conclusions often broadly suggest that increased consumption of plant-based foods leads to health benefits, this generalized perspective may fall short in effectively guiding populations towards healthy eating. Considering dietary diversity and the relatively constant nature of individual daily energy intake, providing specific intake recommendations is essential. Based on dose-response relationships, we have developed a plant-based dietary pyramid tailored for different genders concerning four chronic diseases, aiming to offer practical dietary guidance. Moreover, most existing studies focus on a single chronic disease, while we have considered four, which often co-occur. Therefore, offering plant-based dietary recommendations that simultaneously prevent these four common chronic diseases holds practical significance. We found that intake levels of vegetables, fruits, whole grains, fungi and algae that meet or exceed recommended levels help to prevent the onset of these diseases collectively. Additionally, we suggested that men limit refined grains intake, while women could benefit from higher intakes of nuts and seeds. Individuals may choose to meet or exceed threshold levels based on personal preference. The Dietary Guidelines for Chinese Residents, published in 2016, recommend a daily intake of 300–500 g of vegetables, 200–350 g of fruits, 50–150 g of whole grains, and 25–35 g of nuts and seeds for adults62. Based on our findings, the rounded suggested cutoff values for effective prevention of chronic diseases were ~400–700 g of vegetables, 90–200 g of fruits for men, 90–300 g for women, 80–140 g of whole grains for men, 80–120 g for women, and 10–30 g of nuts and seeds for women. Except for the recommended vegetable intake, which is higher than the guidelines, the suggested intake levels for other plant-based foods fall within the ranges specified by the Dietary Guidelines for Chinese Residents.
Moreover, the current study reveals that the average intake of tubers and legumes exhibits varied dose-response associations with different chronic disease risks. Specifically, the consumption of tubers is inversely related to the risk of hypertension and diabetes, yet shows a positive association with stroke. Legume intake is negatively associated with hypertension, although its relationship with stroke, heart attack, and diabetes varies by gender. The effect of tubers on chronic diseases remains contentious. For instance, tubers are high in potassium, which is generally linked to a reduced risk of hypertension and stroke63. However, Larsson et al. found no association between tuber intake (specifically potatoes) and CVDs64, and other studies suggest that higher tuber consumption may increase hypertension risk63. Similarly, the current study reports inconsistent findings regarding legume intake65,66. Particularly premenopausal women may derive more benefit from tuber consumption due to the protective effects of estrogen against CVDs67,68. Furthermore, different methods of tuber preparation are associated with varying disease risks69. The diverse effects of legumes could be attributed to differences in genetic background, metabolic profiles, or digestive capacity, which may affect how legumes impact cardiovascular health. For example, certain individuals might be sensitive to specific legume components, leading to adverse reactions70,71. Consequently, further research is necessary to elucidate these complex relationships.
Our study has several strengths. Firstly, it addresses the assumption that food intake remains constant during long-term follow-up14 and challenges the notion of a linear relationship between dietary consumption and disease risk17, which is prevalent in current cohort studies investigating the association between plant-based foods and chronic diseases. Our study suggests that plant-based food intake can change significantly over time and that the mechanisms affecting chronic disease risk are complex and do not always follow a linear pattern. To address these issues, we used more appropriate statistical methods, such as RBW and RCS, to draw reliable real-world conclusions. Secondly, we used dose-response curves to determine feasible dietary guidance. Numerous studies have used medians or quartiles to categorize continuous food intake, concluding that consuming more of certain plant-based foods is healthier. However, the appropriateness of median or interquartile cutoffs is controversial72. Thus, our application of dose-response curves allows us to identify the optimal intake levels for specific foods. Thirdly, we extended our analysis to four common chronic diseases and constructed a chronic disease-specific plant-based food pyramid, finding that a diet rich in vegetables, whole grains, fruits, and fungi and algae reduced the risk of all four chronic diseases simultaneously. This finding provides more practical and comprehensive dietary advice for the general population. Fourthly, gender-specific dietary influences were addressed based on the identified gender differences in dietary preferences18 and in the etiology and incidence of chronic disease19,20,21. The new insights revealed that men can moderately incorporate refined grains into their diets, whereas women should increase their intake of nuts and seeds to reduce chronic disease risk. Fifthly, our study provides a more accurate identification of the dose-response relationship between specific plant-based foods and chronic disease risk, thereby addressing the limitations inherent in subjective dietary scoring systems, such as the Healthy Eating Index and Alternative Healthy Eating Index73, which tend to oversimplify complex dietary patterns and may overlook subtle variations and individual habits. Finally, we conducted a sensitivity analysis on the dose-response relationship using a dataset without imputed missing values. The results showed strong consistency between the datasets with and without imputation, with both displaying similar cutoff values overall.
This study has several limitations that require attention. Firstly, reliance on participants’ self-reported dietary data introduces potential recall bias, as individuals may inaccurately report their intake due to memory errors or social desirability bias, compromising data accuracy. Secondly, long-term cohort studies inevitably encounter the issue of participant turnover, which may potentially affect the representativeness of the sample and the generalizability of the findings. Thirdly, while we adjusted for a range of potential confounders—including health behaviors—it was not feasible to eliminate all unmeasured confounders. Factors such as food preparation methods and environmental contamination were inadequately addressed in our study. These uncontrolled confounders could have influenced observed associations, thereby constraining the interpretability of our results.
In summary, this long-term cohort study reveals that a higher intake of vegetables and whole grains, along with appropriate consumption of fruits, fungi and algae for both genders, significantly contributes to the prevention of four chronic diseases. Furthermore, it is recommended that men consume refined grains in moderation, while women should prioritize increasing their intake of nuts and seeds. These findings underscore the importance of personalized dietary guidance in optimizing health benefits and effectively preventing and managing chronic conditions. Future research should continue to investigate the impacts of these diets on different genders and health conditions to provide more precise nutritional guidance.
Methods
Study subjects
The CHNS is a prospective cohort study initiated in 1989 and subsequently conducted across nine surveys in 1991, 1993, 1997, 2000, 2004, 2006, 2009, 2011, and 2015. This long-term endeavor serves as an ongoing exploration into the influence of socioeconomic factors, demographic shifts, and dietary behaviors on health outcomes within China. Employing a meticulous multi-stage random-cluster sampling method, participants were recruited from all nine provinces, which collectively represent ~50% of the nation’s population, and encompass diverse rural, urban, and suburban regions. For a detailed overview of the project’s objectives and methodology, readers are referred to the cohort profile74.
Initially, the study enrolled 9960 participants aged ≥ 18 years in the baseline year (2004). Subsequently, individuals with a history of stroke, myocardial infarction, hypertension, or diabetes were excluded from the analysis along with pregnant or breastfeeding women at baseline. Additionally, participants who were lost during follow-up were also excluded. The final cohort comprised 6317 subjects meeting the eligibility criteria (2947 men and 3370 women). The participant flow chart can be found in Supplementary Fig. S2.
The study was conducted according to the guidelines of the Declaration of Helsinki, and received approval from the institutional review committees of the University of North Carolina at Chapel Hill and the Chinese Institute of Nutrition and Food Safety, China Center for Disease Control and Prevention. All participants provided written informed consent.
Outcome measurement
The study assessed various health outcomes including hypertension, stroke, myocardial infarction, and diabetes. Participants were queried regarding any prior diagnosis of these conditions by a doctor or healthcare professional. Those who self-reported medication usage for diabetes or hypertension were also considered. Additionally, participants were seated and rested for at least 10 minutes before having their arterial blood pressure meticulously measured three times on the right arm using a mercury sphygmomanometer. The cuff was positioned at heart level to ensure accuracy. Subsequently, the average of these three blood pressure readings was calculated and used to determine hypertension status, further ensuring the precision of the measurements. Hypertension was defined following the 2018 Chinese guidelines for hypertension management as systolic blood pressure (SBP) ≥ 140 mmHg and/or diastolic blood pressure (DBP) ≥ 90 mmHg, or recent utilization of antihypertensive medication within the past 2 weeks75.
Assessment of plant-based foods
As the dietary data for the 2015 wave were not released, we utilized plant-based food exposures from four subsequent waves spanning from 2004 to 2011. At the individual level, dietary assessments entailed three consecutive 24-h recalls, during which trained interviewers recorded all food consumption, both at home and outside, using food models and pictures. Household-level inventory weighing was conducted over the same three-day period. To ensure equal distribution across the week for each sampling unit, these three days were randomly allocated from Monday to Sunday. Changes in household food inventory from the beginning to the end of each day were monitored using a weighing scale. Discrepancies between the average daily dietary intake (measured in g/day) from the household survey and the 24-h recall were detected and resolved by revisiting and reconciling data at both levels. The classification of plant-based food groups, such as refined grains, whole grains, vegetables, tubers, fruits, fungi and algae, legumes, and nuts and seeds, was determined based on the dietary consumption data utilizing the Chinese Food Composition Table 200476.
Potential covariates
The CHNS collected self-reported demographic information including age, gender, residential area, the highest level of education attained, annual income, sleep duration, smoking, and drinking status through interviewer-administered questionnaires in each survey wave. Body mass index (BMI) was calculated by dividing weight in kilograms by height in square meters. The weight and height measurements of all participants were collected by trained healthcare professionals using calibrated equipment (Seca 880 scales and Seca 206 wall-mounted metal tapes, Seca North America). The modified short-form International Physical Activity Questionnaire (IPAQ) was utilized to assess physical activity level, and the weekly total metabolic equivalent task (MET) was calculated77. Supplementary Table S4 describes the definitions of covariates in detail.
Statistical analysis
For each survey wave, we calculated the mean and standard error for continuous exposures, as well as percentages for binary exposure variables. Baseline characteristics were compared by gender using either the Student’s t-test or the chi-square test. The cumulative incidence was calculated by dividing the number of new cases observed during the observation period by the total number of individuals at risk at the beginning of the observation period. The generalized estimating equations were employed to assess whether repeated measures of observed variables demonstrated alterations over time and to investigate whether discrepancies in their time trends existed based on gender group78. The time-varying confounders were controlled by constructing RBW22. RBW was a method for constructing weights in marginal structural models to control for time-varying confounders. It simultaneously enforced covariate balancing and minimized entropy conditions on the weights, making it both more efficient and robust compared to traditional methods. Additionally, it simplified the analysis of continuous exposures by eliminating the need for arbitrary quantile binning commonly used in practice. All identified time-varying confounders were used to construct RBW. The RCS model was utilized as a marginal structure model based on RBW to investigate the average dose-response relationship between plant-based food consumption and chronic disease incidence23. When assessing each plant-based food, other plant-based foods were adjusted for as covariates. All covariates identified as time-varying by the generalized estimation equations were included in the construction of the RBW weights. Additionally, time-invariant covariates, such as residential area, along with age—which was time-varying but had fixed values—were adjusted in the RCS.
The outcomes data were complete for all patients, and any missing covariates were imputed using multiple imputations by the fully conditional specification method79,80,81. We performed sensitivity analyses to explore the robustness of the associations between diet and chronic disease. To ensure that the imputation of missing data did not affect our research results, we used the original unimputed data and applied the same analytical procedures as before to verify the stability of the association between diet and chronic disease.
Data cleaning, consolidation, and imputation were completed using SAS software version 9.4 (SAS Institute Inc., Cary, NC, USA). Statistical tests were performed using R software (version 3.6.1). The statistically significant difference was defined as P < 0.05, and the 95% confidence interval (CI) of the hazard ratio (HR) not including 1. All P values were two-tailed.



Responses