An analysis on the role of glucagon-like peptide-1 receptor agonists in cognitive and mental health disorders
Main
Glucagon-like peptide-1 receptor agonists (GLP-1RAs; also known as ‘incretin mimetics’) are a class of medications licensed for the treatment of type 2 diabetes mellitus (T2DM) and obesity1. These drugs fall within two categories: human GLP-1 backbone agents (that is, albiglutide, dulaglutide, liraglutide and semaglutide) and exendin-4 backbone agents (that is, exenatide, lixisenatide and tirzepatide—the latter activating both GLP-1 and glucose-dependent insulinotropic polypeptide (GIP) receptors)1. GLP-1 and GIP are incretin hormones that stimulate insulin secretion after an oral glucose load by binding GLP-1R, but both are rapidly inactivated by the enzyme dipeptidyl peptidase-4 (DPP-4). GLP-1RAs activate GLP-1R similarly to GLP-1, but they are resistant to the activity of DPP-4. Ultimately, GLP-1RAs enhance insulin excretion, leading to the inhibition of glucagon production by pancreatic α-cells when blood sugar levels are high as well as a decrease of pancreatic β-cell apoptosis and an increase in their proliferation. Furthermore, these drugs delay gastric emptying and appear to increase satiety due to direct activity on the hypothalamus and brain stem. Numerous studies have investigated the expression patterns of endogenous GLP-1 and GLP-1R in the central nervous system (CNS) and the peripheral nervous system, with a consensus that these are expressed on neurons and found in most areas of the brain and gut–brain axis2. Specifically, beyond the enteroendocrine L-cells of the intestine, GLP-1 is also produced as a neuropeptide by the pre-proglucagon neurons in the brain stem3. Although some GLP-1RAs do not seem to naturally cross the blood–brain barrier, they may still reach relevant brain areas via circumventricular sites and, possibly, via active transporters4,5. The implications of centrally produced, neuromodulatory GLP-1 in the context of GLP-1RAs are uncertain, as the degree to which signals from pre-proglucagon neurons/endogenous GLP-1 system and GLP-1RA activity converge on shared downstream targets is unclear6 and may in fact occur independently7. Most GLP-1RAs, aside from a new oral formulation of semaglutide (Rybelsus tablets), are administered subcutaneously via pen-like devices (once daily to once weekly) due to poor oral bioavailability, and all are renally excreted1. Nausea, vomiting, dyspepsia and diarrhea are common side effects; uncommon or unconfirmed more severe reactions may include acute kidney injury, hypoglycemia, thyroid neoplasia and acute pancreatitis.
Because of their substantial benefit on some of the most highly prevalent disorders worldwide, GLP-1RAs have been hailed as ‘game changers’8,9 and ‘breakthrough drugs’10, with an estimated market value of US$22.4 billion in 2022 and a compound annual growth rate of around 9.6% between 2023 and 203211. They are being extensively used (that is, prescribed both in-label and off-label) and misused (that is, obtained without prescription online) for weight loss in the general population, under the limelight of a so-called media frenzy12. Such widespread usage has led to a severe and prolonged international shortage of these drugs13,14, with consequent lack of access to treatment for patients with diabetes15 and the urgent need to issue guidelines for alternative treatments16.
Several major randomized controlled trials (RCTs) have confirmed the efficacy and safety of GLP-1RAs in adults with diabetes17 and obesity18, and more recently in child and adolescent populations living with obesity19,20. Importantly, these medications lead to a considerable reduction of cardiovascular morbidity21 and population-level all-cause mortality22. Other trials are investigating their metabolic and non-metabolic (that is, disease specific) effects in a variety of chronic illnesses including kidney and liver disorders, Alzheimer’s dementia and schizophrenia23,24.
On the basis of several putative modes of action under investigation (for example, neuroprotective and anti-inflammatory properties, regulation of reward pathways), there is an emerging consensus that GLP-1RAs could be repurposed for use in neuropsychiatric conditions25,26,27,28,29,30,31,32. In this comprehensive overview (see Methods and the search methodology in Supplementary Section 1), we aim to identify and describe pre-clinical, mechanistic and clinical studies on the effects of GLP-1RAs in cognitive and mental health disorders, and to provide a summary of available evidence and future perspectives. Evidence was reported according to the neuropsychiatric condition under investigation: cognitive disorders (dementia, Parkinson’s disease), substance-use disorders, psychotic disorders, mood and anxiety disorders, and eating disorders—each subdivided into pre-clinical and mechanistic evidence, and clinical evidence, the latter reported following a hierarchy of evidence (that is, meta-analyses, clinical trials, observational studies, case series). Miscellaneous studies (for example, reporting on any psychiatric adverse outcomes) as well as ongoing and planned trials are reported in Supplementary Sections 2 and 3, respectively.
Results
The initial search yielded 23,496 records of which 6,821 were duplicates. Screening of 16,675 titles and abstracts led to the removal of 15,778 non-relevant studies. A further 523 articles were excluded on eligibility assessment of 897 full texts. Eventually, 374 studies were eligible for inclusion in the review (Extended Data Fig. 1).
Cognitive disorders
Pre-clinical and mechanistic studies
Our search retrieved a high number (N = 189) of pre-clinical or mechanistic studies assessing the possible effects of GLP-1RAs on cognitive disorders, which cannot be described in the main text of this article due to space constraints (Supplementary Section 4). Here we therefore report only the five more recent and inclusive reviews that summarize such evidence. A meta-analysis of 26 animal studies showed that GLP-1RAs improved learning and memory in rodent models of Alzheimer’s disease, possibly by decreasing brain levels of Aβ-amyloid deposition and phosphorylated tau33. There is also evidence for mechanisms involving a reduction of neuroinflammation, an increase in synaptic functioning, as well as the restoration of brain pathways of insulin signaling that may lead to improved memory formation and therefore a positive effect in Alzheimer’s disease and Parkinson’s disease34. Brain insulin resistance may indeed play a role in the pathophysiology of cognitive disorders, and addressing this may be a mechanism through which GLP-1RAs act pro-cognitively35. GLP-1R activation of neuroprotective pathways in neurons, microglia and astrocytes has also been reported: improvements in overall cognition, learning and motor function potentially associated with GLP-1RA administration in Alzheimer’s disease and Parkinson’s disease may be mediated not only by their amyloid pathology-ameliorating properties (Aβ, tau and α-synuclein), but also the suppression of Ca2+ deregulation and endoplasmic reticulum stress, anti-inflammatory activity, blockage of oxidative stress, mitochondrial dysfunction and apoptosis pathways, enhancements in the neuronal insulin sensitivity and energy metabolism, functional improvements in autophagy and mitophagy, elevated brain-derived neurotrophic factor and glial cell line-derived neurotrophic factor synthesis, and neurogenesis36. Other neuroprotective mechanisms potentially involved in the treatment of cognitive disorders as well as cerebrovascular disease and epilepsy suggest that GLP-1RAs can enhance the viability of neurons and restore neurite outgrowth by stimulating neurotrophic factors, thus increasing subventricular zone progenitor cells, decreasing apoptosis and the level of pro-inflammatory factors, and strengthening the blood–brain barrier37.
Clinical studies
A total of 22 completed clinical studies were identified (Table 1 and Extended Data Tables 1 and 2), with another 8 clinical trials still ongoing (Supplementary Section 3).
Four meta-analyses pooled both randomized and non-randomized evidence to assess the effects of GLP-1RAs on dementia risk or cognitive outcomes from studies conducted in people with a background diagnosis of T2DM or obesity38,39,40,41. A meta-analysis of 5 RCTs42,43,44,45,46 comprising 7,732 adults with T2DM did not observe any effect on cognition, as measured via mini-mental state examination (MMSE) or Montreal cognitive assessment (MoCA), of GLP-1RAs over several months compared with the baseline38. A pooled analysis of 3 longer-term RCTs22,47,48 following 15,820 patients with T2DM up to 3.8 years showed a reduced risk of dementia for semaglutide and liraglutide compared with placebo39. The same paper also included a nested case-control component of 120,054 patients with T2DM followed for 7.4 years and observed a lower association between dementia and exposure to GLP-1RAs compared with other antidiabetics39. This finding was further supported when pooled with further observational data49,50 to a total of 210,521 people with T2DM up to 7.4 years on any GLP-1RA40. Finally, a recent network meta-analysis that compared cognitive outcomes with various antidiabetic agents in patients with type 2 diabetes observed that GLP-1RAs ranked second after sodium-glucose cotransporter-2 inhibitors for reducing dementia risk. However, this meta-analysis included only one RCT43 and one case-control study51 for GLP-1RAs (but not the more recent semaglutide)41.
All clinical trials for dementia outcomes identified by our search42,43,44 had been included in the meta-analyses above. Among these trials, one involving 36 patients with T2DM did not show any difference from baseline on the MMSE and MoCA after liraglutide at 16 weeks—although all participants had preserved cognitive function at baseline, while an improvement on tests for delayed memory (possibly mediated by left hippocampal activation), attention and executive function was noted42.
However, we further retrieved four RCTs in Parkinson’s disease looking at both motor and non-motor outcomes, but results were inconsistent depending on the different scales used within the same trial; overall, one showed a more beneficial profile52, while the other three did not find any consistently positive effect53,54,55.
Among the observational studies39,45,46,49,50,51 comprised by the meta-analyses, two are worth a separate mention. One observed a positive association between liraglutide use at 12 weeks and improved MMSE in 47 adults with T2DM, which correlated with increased task (verbal fluency)-based activation of the dorso-lateral prefrontal and orbitofrontal cortex, while several other cognitive tests were not affected45. In another study, the same treatment in 19 participants with obesity and diabetes was associated with an improved MoCA score, olfactory test total score and enhanced odor-induced right parahippocampus activation46. Moreover, we retrieved other relevant records56,57,58: two large (N = 133,318 and N = 342,608, respectively) cohort studies in people with diabetes across 6–13 years noted a beneficial association between GLP-1RA prescriptions compared with non-prescription and lower diagnoses of dementia57,58, while a small (N = 154 patients with T2DM) and shorter (~12 months) cross-sectional investigation of GLP-1RAs in addition to metformin, compared with metformin alone, observed better MoCA scores in the former group56.
No studies investigating possible interactions between GLP-1RAs and antidementia drugs were found.
In summary, there is a considerable number of clinical studies reporting the potential benefit of GLP-1RAs for use in cognitive disorders, including dementias and Parkinson’s disease, although the majority are observational and can only suggest association. Such evidence, however, is supported by many relevant pre-clinical or mechanistic studies highlighting the neuroprotective and anti-inflammatory activity of these medications. Conversely, we found little evidence that GLP-1RAs may cause or exacerbate cognitive impairment, which is of importance to patients who may need to take these medications for their currently licensed (and expanding) indications.
Substance-use disorders
Pre-clinical and mechanistic studies
A large body of pre-clinical and mechanistic literature is available regarding the putative effects of GLP-1RAs on substance misuse (Supplementary Section 5): 24 for alcohol59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82, 8 for opiates63,83,84,85,86,87,88,89, 16 for stimulants, including cocaine and amphetamines90,91,92,93,94,95,96,97,98,99,100,101,102,103,104,105, and 4 for nicotine106,107,108,109. A large proportion of these studies reported on the impact of GLP-1RAs on dopaminergic neurotransmission responsible for reward processing—which could contribute to their efficacy as anti-obesity medications by means of a reduction of food-related incentive110.
Alcohol
Several studies investigating exendin-4, liraglutide, dulaglutide and semaglutide in rats and mice found a decrease in alcohol use, which was mediated by mesolimbic dopamine pathways involving the nucleus accumbens, the ventral tegmental area and the ventral hippocampus, the dorso-lateral septum, and the nucleus of the solitary tract59,60,61,63,64,65,66,67,68,69,72,74,75,76,77,79,80,81,82,106. One study replicated such positive findings in non-human primates78. It has also been suggested that GLP-1RAs may affect alcohol misuse and withdrawal symptoms by modulating anxiogenic mechanisms in rats73. Another study showed no synergistic activity of the antismoking agents, bupropion and varenicline, when administered to rats in addition to semaglutide to reduce alcohol intake62. Finally, a post-mortem analysis of human brain samples showed increased hippocampal expression of genes encoding for GLP-1R in individuals with severe alcohol-use disorder compared with controls71.
Opiates
Exendin-4 and liraglutide reduced cue- and drug-induced opiate-seeking behavior in rats and mice across several studies83,84,85,86,87,88. Only one study did not identify any benefit of GLP-1RAs in animal models of opiate misuse, although this same study had shown a positive effect for alcohol misuse63. An investigation of the dual GLP-1R and neuropeptide Y2-receptor agonist, GEP44, found that this drug attenuated opioid taking and seeking at a dose that did not suppress food intake in rats89.
Cocaine and amphetamines (stimulants)
All animal studies retrieved for stimulants misuse involved exendin-4 among GLP-1RAs and highlighted a reduction of cocaine and amphetamines intake and end effects (for example, increased locomotor activity) via modulation of dopaminergic transmission in areas including the nucleus accumbens and the ventral tegmental area91,92,93,94,96,97,98,99,100,101,102,103,105, as well as modulation of inflammatory mechanisms104. One genetic study described an enhanced effect on cocaine use in GLP-1R knockout mice achieved via viral-vector delivery of the gene encoding for GLP-1R to the dorso-lateral septum95. In humans, intravenous cocaine injection was shown to decrease plasma GLP-1 concentration, while endogenous GLP-1 was associated with subjective responses to cocaine90.
Nicotine
Only two pre-clinical investigations on the effects of GLP-1RAs in nicotine misuse were retrieved, both showing less nicotine use and related outcomes (for example, withdrawal-induced hyperphagia) for liraglutide108 and exendin-4 possibly related to dopamine regulation106. Moreover, liraglutide appears to diminish nicotine-induced dopamine signaling in the nucleus accumbens107. An optogenetic stimulation of GLP-1Rs in habenular circuits was also shown to abolish nicotine reward and decrease nicotine intake in mice109.
Clinical studies
Compared with the considerable amount of pre-clinical and mechanistic research reported above, we identified few clinical studies of GLP-1RAs for substance-use disorders (Table 2): three for alcohol111,112,113, one for cannabis114, two for cocaine115,116 and two for nicotine117,118, while no article about opiates or amphetamines was retrieved. However, we found another nine clinical trials that are ongoing: six for alcohol, one for opiates and two for nicotine (Supplementary Section 3).
Alcohol
A recent 26-week RCT of 127 people with alcohol-use disorders found a positive effect of exenatide compared with placebo in people with obesity only111. A similar beneficial association was seen in an observational study of semaglutide in 83,825 patients with obesity and 598,803 patients with T2DM over 12 months112, as well as in 87,676 new users of GLP-1RAs or DPP-4 inhibitors over 4 years113.
Cannabis
While no pre-clinical or mechanistic study has considered GLP-1RAs for cannabis misuse so far, a large epidemiological investigation has recently noted an association between semaglutide use and fewer cannabis-use disorders in both patients with T2DM (N = 596,045) and patients with obesity (N = 85,223) over a 1-year follow-up114.
Cocaine
Only limited clinical evidence is available for GLP-1RAs in cocaine misuse: a small (N = 13) proof-of-concept trial across 2 days showed that exenatide compared with placebo did not reduce the number of self-administered cocaine infusions115, while a case series of 3 individuals with cocaine-use disorder highlighted the feasibility and safety of using the same drug over 6 weeks, although no efficacy measures were reported116.
Nicotine
A trial of 84 smokers with prediabetes and overweight found that exenatide was superior to placebo in terms of nicotine abstinence rates at 6 weeks118. However, a more recent RCT of 255 adults with nicotine dependence did not show any effect of adjunctive dulaglutide compared with standard of care (that is, behavioral counseling with varenicline) on cigarette abstinence over 12 weeks of treatment117.
No studies investigating possible interactions between GLP-1RAs and anti-addiction drugs were found.
Overall, compared with the large and growing amount of pre-clinical and mechanistic evidence highlighting the reward-modulating and thus potentially anti-addictive properties of GLP-1RAs, only a few studies have investigated thus far the potential use of these medications in clinical populations with alcohol- or other substance-use disorders. Because this is an area with notable unmet needs, especially in terms of pharmacological treatment options, further research investment is warranted.
Psychotic disorders
Pre-clinical and mechanistic studies
Several pre-clinical and mechanistic studies examined the possible effects of GLP-1RAs in psychotic disorders (Supplementary Section 5). In animal models of psychosis, liraglutide administration consistently led to a reduction of psychotic-like behavior119,120,121, which was also associated with increased brain-derived neurotrophic factor, CREB/p-CREB, and Trk-B expression in the hippocampus and prefrontal cortex120, and reduced serum and hippocampal tumor necrosis factor and oxidative stress121.
Several animal studies investigated the effects of liraglutide122,123,124,125,126,127 and exendin-4 (refs. 126,128) on metabolic side effects (for example, hyperglycemia, hyperlipidaemia, weight gain) of atypical antipsychotics including olanzapine, quetiapine, brexpiprazole and clozapine. All122,124,125,126,127,128 but one123 study showed a benefit on metabolic parameters. Two studies also showed concomitant improvements in cognitive measures of recognition and working memory122 and depressive-like behavior in rats administered antipsychotics127. A similarly positive effect on glucose metabolism was observed in mice exposed to clozapine and the non-peptidic GLP-1RA Boc5 (ref. 129).
Three studies explored mechanistic associations between GLP-1 functioning, psychosis and antipsychotic treatment in humans. Low levels of serum GLP-1 were reported in 260 patients with a diagnosis of first-episode psychosis compared with healthy controls130. Serum GLP-1 levels showed direct proportionality with several metabolic risk markers (that is, body mass index (BMI), leptin, insulin) over 109 men diagnosed with schizophrenia and on clozapine, while this association was not observed in women131. An exploratory analysis of genetic data of patients from the Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE) trial showed that different haplotypes encoding for GLP-1R correlated with variable response rates to antipsychotic medications132.
Clinical studies
All 23 relevant clinical studies for this section focused on the effects of GLP-1RAs on cardiometabolic parameters in people with schizophrenia-spectrum disorders on antipsychotics, apart from a secondary analysis investigating cognitive and mental health outcomes133 (Table 3 and Extended Data Tables 3 and 4). This also applied to another five ongoing studies identified (Supplementary Section 3).
The four meta-analyses134,135,136,137 were successively updated to incorporate upcoming trials, so that the most recent134 included seven RCTs138,139,140,141,142,143,144. This meta-analysis showed that, over 398 patients with schizophrenia treated with antipsychotic followed up between 12 and 24 weeks, the GLP-1RAs liraglutide and exenatide were superior to placebo for body weight, waist circumference, BMI and blood pressure134. The meta-analysis by Wang and colleagues137 included an unpublished trial (NCT00845507145) that was not part of the more recent meta-analysis by Khaity and colleagues134. For this RCT, we identified a conference abstract that similarly reported a positive effect of exenatide on weight reduction and BMI146.
As mentioned, a secondary analysis of an RCT assessing the cardiometabolic effects of exenatide in 40 people with schizophrenia140 also looked at measures of cognition and psychosocial functioning (that is, Brief Assessment of Cognition in Schizophrenia, Rey–Osterreith Complex Figure Test, Short-Form Health Survey, Personal and Social Performance Scale, Positive and Negative Syndrome Scale), but found no effect for this GLP-1RA compared with placebo over 3 months133. All other trials retrieved139,140,141,142,143,144,146,147 investigated cardiometabolic parameters and were included in the meta-analyses above134,137,138.
Three small cohort studies148,149,150 examined associations between GLP-1RA use and metabolic changes in adults with a diagnosis of schizophrenia and comorbid diabetes and/or obesity on antipsychotics. Of these, two studies (N = 16 and N = 46, respectively) observed a positive association between the use of exenatide, liraglutide or dulaglutide and weight loss as well as HbA1c at 16 weeks149 and 1 year150, while for the smaller one (N = 7) this association was not significant148.
All case series and reports151,152,153,154,155 reported better metabolic outcomes in patients with comorbid severe mental illness and diabetes and/or obesity who were concomitantly treated with antipsychotics and GLP-1RAs. A qualitative sub-study of the trial by Whicher and colleagues144 over 17 patients with overweight or obesity and schizophrenia-spectrum disorders found that most of the interviewees and their clinicians had had positive experiences regarding GLP-1RA administrations.
Compared with other neuropsychiatric illnesses, most studies on the effects of GLP-1RAs in psychotic disorders seem to have focused so far on their potential use to counteract the cardiometabolic side effects due to antipsychotic medications. While this is a key research area, we propose that further investigations should verify whether GLP-1RAs may also affect cognitive and behavioral symptoms seen in psychosis, as suggested by their potential to influence neurobiological (for example, immune function) and neuropsychological (for example, reward) mechanisms that are known to be disrupted in psychotic illness.
Mood and anxiety disorders
Pre-clinical and mechanistic studies
Articles relevant to this section mainly addressed depressive and anxiety conditions, while only two pre-clinical studies investigated the effect of GLP-1RAs in bipolar disorder (Supplementary Section 5). In animal models of mania, liraglutide augmented the activity of the mood stabilizers sodium valproate156 and lithium157. This effect appeared to be mediated by antioxidant mechanisms involving GSK3β phosphorylation156, and it was also associated with a reduction of measures of memory impairment in mice157.
Several animal studies were found to be relevant for depression and anxiety158,159,160,161,162,163,164,165,166,167,168, although with conflicting results. Two studies on exenatide162,166 and one on liraglutide162 showed no effect of these GLP-1RAs on depression-like behavior. One of these studies also failed to identify any change in anxiety-like behavior162, while two further studies employing exendin-4 observed an anxiogenic effect following acute administration158,169. Intriguingly, one of these studies also showed that longer administrations can lead to a normalization of anxiety and a dissociable improvement in depression-like behavior158—a pattern that resembles of the mechanisms of action of conventional antidepressants and that may be further suggestive of the activity of GLP-1RAs on the serotonin system158. Three further articles reported a beneficial effect of liraglutide on depression-like165 as well as anxiety-like behavior164,167 in rats and mice, possibly mediated by neuroprotective mechanisms in the hippocampus164,167, and improved cognitive function165. Similarly, both lixisenatide163 and dulaglutide160 administration led to positive changes in different paradigms of depression induced in mice.
Two studies investigated animal models of comorbid depression and epilepsy159,161: one showed that exendin-4 led to an increase in frequency of absence seizures as well as depressogenic and anxiogenic responses159, while the other saw a decrease of depression-like behavior for liraglutide irrespective of concurrent use of the antiepileptic levetiracetam161. In an animal model of depression and diabetes, however, exendin-4 led to antidepressant-like effects, which was associated with changes in microglial function168.
Finally, we identified six papers describing favorable associations between GLP-related molecules (that is, geniposide, GLP2, puerarin) and reductions in depression-like behavior170,171,172,173,174,175.
One study explored mechanistic associations between GLP-1 functioning and mood disorders in humans: a post-mortem investigation showed that, compared with healthy controls, patients who had been diagnosed with mood disorders had lower expression of the gene encoding for GLP-1R in the dorso-lateral prefrontal cortex and the hippocampus, whereas this association was not observed in the brain tissue of people with schizophrenia176. Furthermore, a recent resting-state functional magnetic resonance imaging (MRI) analysis of 18 women with obesity or polycystic ovary syndrome (PCOS) randomized to either 16-week semaglutide or placebo showed no significant changes in brain regions associated with depression and suicidality177.
Clinical studies
We split this section between studies of GLP-1RAs in people with mood disorders and studies of mood symptoms in patients with other medical conditions taking GLP-1RAs (Tables 4 and 5, and Extended Data Tables 5 and 6).
Only four clinical studies specifically examined GLP-1RAs in mood disorders (Table 4). One non-randomized open-label study, published over 2 separate articles, showed that 4-week liraglutide led to an improvement in a test of executive functioning (and possibly other cognitive measures)178 and related increase in fronto-striatal volumes179, partly moderated by BMI and insulin resistance changes, in 19 people diagnosed with bipolar disorder or major depression. A historical cohort investigation of 29 patients with comorbid mood disorder and obesity noted that liraglutide-induced weight loss over 6 months was not associated with changes in psychiatric symptoms, although less than half of the study population completed the study period180. Conversely, some case reports for exenatide181 and semaglutide182 described onset or relapse of depressive symptoms, which resolved when the GLP-1RAs were stopped181,182 and recurred on medication rechallenge181.
In contrast, we found a larger amount of evidence over 26 studies assessing depressive symptoms in populations with comorbid physical health conditions undergoing GLP-1RA treatment (Table 5). A recent meta-analysis of mixed evidence (5 RCTs52,183,184,185,186 and 1 cohort study187) in 2,071 people with T2DM or Parkinson’s disease suggested antidepressant efficacy of the GLP-1RAs exenatide and liraglutide over 24–52 weeks188. The same finding had been reported by a prior larger meta-analysis (6,914 patients with overweight or obesity and T2DM) over 8 studies184,185,189,190,191,192,193,194, but only when the largest study that also included non-diabetic participants193 was excluded in a sensitivity analysis195. In fact, the omitted study was a pooled analysis of 5 RCTs196,197,198,199,200 of 5,325 patients with obesity followed for up to 3 years, which had shown that liraglutide was no different from placebo for depressive symptoms as scored on the Patient Health Questionnaire-9, while also highlighting a small increased risk of suicidal behavior193.
The above meta-analyses comprised all clinical trials we could retrieve with our search52,183,184,185,186,189,191,196,197,198,199,200. One of these trials also assessed anxiety symptoms and found no effect of liraglutide compared with placebo over 26 weeks in 80 patients with comorbid T2DM and obesity who had previously undergone bariatric surgery186.
Of the cohort studies already included above187,190,192, two report additional results of relevance. An early cohort study on a small number of patients with diabetes (N = 138) saw reduced depression scores at 18 months in people exposed to exenatide compared with insulin independently from BMI changes190. This result was replicated in a similar but larger investigation (N = 1,735) comparing all available GLP-1RAs versus non-GLP-1RA antidiabetics, with this antidepressant association possibly correlating with changes in markers of systemic inflammation (that is, high-sensitivity C-reactive protein)192. We also identified several further observational investigations. A recent and more extensive (N = 10,690 people with diabetes followed up over 6–7 years) historical cohort study observed a reduced association between GLP-1RA use compared with non-use for depressive and, more pronouncedly, anxiety disorders incidence, especially in women32. However, another study with similar design did not see any association between GLP-1RA exposure and changes in new-onset depression or self-harm over 16,910 patients with diabetes over approximately 1 year of follow-up201. Two 10-year case-control studies over very large samples of people with diabetes (N = 360,205 and N = 73,869, respectively) equally observed no association between GLP-1RA use and incident depression202,203. Also, a small cross-sectional study of 36 women with PCOS noted no changes in depression scores associated with liraglutide use over 6 months204, while another reported worsening depressive symptoms, which correlated with higher perceived stress scores, in 43 exenatide users with diabetes and obesity against non-users at 3 months205. Finally, following recent concerns by regulatory agencies regarding a potential increase in suicidal behavior associated with GLP-1RAs206, we found 1 recent pharmacovigilance report showing 0.6% suicidal events among 41,236 safety reports for these medications207 and an emulated target trial of 86,418 older adults with T2DM that did not identify any difference in suicidal ideation or behavior between GLP-1RAs and other antidiabetic medications over 1.5 years208. Instead, a historical cohort study of over 200,000 electronic health records found a reduced association between semaglutide use and suicidality in both people with T2DM and obesity at 1 year209.
We did not identify any study that specifically addressed potential interactions between GLP-1RAs and frequently used antidepressant medications.
Although several studies have investigated GLP-1RAs across mood and anxiety disorders, evidence appears mixed, as beneficial, harmful and null effects have all been reported for depressive symptoms and suicidality. Furthermore, the evidence base for the mechanisms possibly involved in the mood-regulating properties of these medications appear more tentative and would benefit from a more in-depth assessment. At present, clear clinical recommendations regarding the safety of GLP-1RAs for people with pre-existing depression or suicidal behavior cannot be made.
Eating disorders
Pre-clinical and mechanistic studies
We retrieved only a few pre-clinical and mechanistic articles relevant to GLP-1RAs for eating disorders (Supplementary Section 5). Higher GLP-1 levels inversely correlate with binge-like eating in animals210,211, and binging behavior is associated with lower GLP-1R in the nucleus of the solitary tract212. The GLP-1RA exendin-4 reduced binge-like feeding in rats via action on μ-opioid receptors in the nucleus accumbens213.
Clinical studies
Despite their thriving role in the treatment of obesity214, only seven studies investigated the effects of GLP-1RAs in eating disorders (Table 6), including some on their psychopathology in comorbid obesity215,216,217 and others specifically in binge-eating disorder (BED)217,218,219,220, and we could not find any ongoing trial in this area. For a comprehensive review of the anti-obesity effects of GLP-1RAs, which is beyond the purpose of this article, see ref. 221.
A single-arm trial showed that liraglutide reduced, from pre-exposure to 12 weeks post-exposure, the occurrences of uncontrolled and emotional eating in 36 women with obesity and PCOS216. Similar results were observed in a later study for 69 adults with obesity using semaglutide217. However, a long-term exploratory RCT in 150 people with obesity found that differences in eating disorders’ psychopathology scores were not maintained at 52 weeks when liraglutide in combination with behavioral therapy was compared with behavioral therapy alone215.
An early RCT in 44 patients with obesity and subclinical binge eating showed that liraglutide was better than diet and exercise alone in reducing binge-eating scores at 12 weeks220, but a later investigation of 27 adults with BED comparing liraglutide against placebo did not find any differences in the number of binging episodes over 17 weeks218. Another positive finding was seen in 60 patients with BED and T2DM when dulaglutide, which is not currently licensed for obesity, was compared with placebo at 12 weeks222. Over a longer follow-up of 180 days, a retrospective cohort study of semaglutide still observed lower scores in binge-eating psychopathology than other anti-obesity medications in 48 patients with moderate to severe BED219.
Despite their established role in promoting weight loss, there is a paucity of research investigating the safety or efficacy of GLP-1RAs in people whose eating disorders have a psychopathological component (for example, anorexia nervosa, bulimia nervosa) as conventionally defined by diagnostic manuals. While there may be some resistance to the conduction of clinical trials of pharmacological interventions in these clinical populations, the mechanistic profile of GLP-1RAs clearly suggests that these medications may play a role in the treatment of certain specific eating disorders, such as BED.
Discussion
In this article, we reviewed pre-clinical and mechanistic studies (in vitro, in animal and in human) and clinical studies, leveraging potential translational aspects, on GLP-1RAs across a variety of cognitive and mental health disorders. Overall, we identified 280 pre-clinical and mechanistic studies (Fig. 1 and Supplementary Sections 4 and 5) and 96 clinical studies (Tables 1–6, Fig. 2, Extended Data Fig. 1, Extended Data Tables 1–6 and Supplementary Section 2), with a clear trend of growing relevant literature over the past few years as the use of these medications becomes more widespread and their indications expand far beyond the initial intentions of the manufacturers223. Some key messages and common themes emerge.

The potential usefulness of GLP-1RAs in psychiatric disorders may be underpinned by their multimodal actions in the CNS and beyond: decreasing inflammation and oxidative stress, reducing neural insulin resistance, modulating neural metabolism and microglial function, and regulating key neurotransmitter pathways. In addition, the cardiometabolic benefits of these agents could lead to improved morbidity and mortality outcomes in this patient population. GLP-1RA effects on higher-order neuropsychological processes, on stress responses or on the gut microbiome remain to be explored. Upward arrows indicate an increase, downward arrows indicate a decrease, the tilde indicates regulates and the question mark indicates uncertain. 5HT, 5-hydroxytryptamine; BBB, blood–brain barrier; BDNF, brain-derived neurotrophic factor; CV, cardiovascular; DA, dopamine; GI, gastrointestinal; HPA, hypothalamus–pituitary axis.
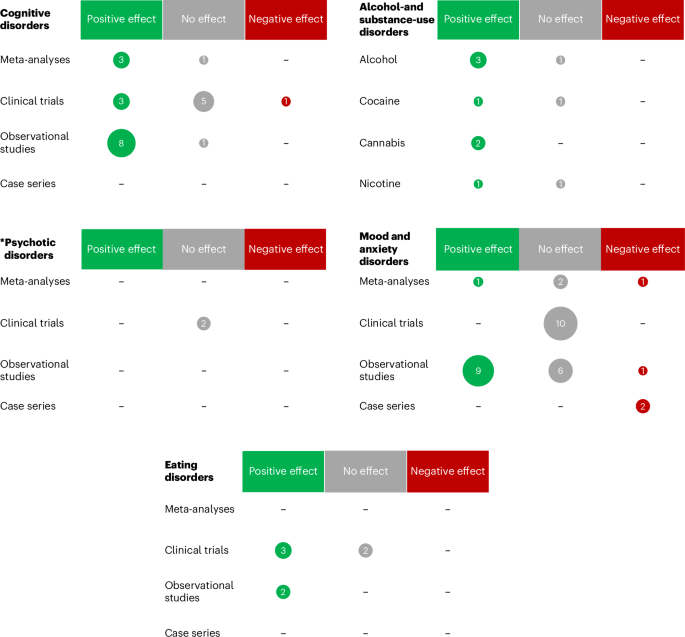
Green, positive effect/association; gray, no effect/association; red, negative effect/association; the area of each circle is proportional to the number of studies. The asterisk indicates that it does not include studies of metabolic effects of GLP-1RAs in people with psychotic disorders, which would not be in line with the psychiatric outcomes reported for all other disorders.
First, there is supporting evidence for the safety of GLP-1RAs across the board of cognitive and mental disorders, as we retrieved very few studies44,159,181,182,193,205 suggesting worse neuropsychiatric outcomes associated with these medications (Tables 1–6, Fig. 2, Extended Data Tables 1–6 and Supplementary Section 2). A recent meta-analysis of 31 RCTs including 84,713 patients comparing any GLP-1RA against placebo found no difference in the incidence of adverse neuropsychiatric events over >1 year224, and several pharmacovigilance studies published over the past year have been in line with such results225,226,227,228,229 (Supplementary Section 2). Publication bias and poor recording of adverse events, which is common in clinical trials, may however explain such paucity of safety signals. In July 2023, the European Medicines Agency206 and the UK Medicines and Healthcare products Regulatory Agency (MHRA)230 started a review of these medications’ safety following reports of worsening mood and suicidal behavior observed in GLP-1RA users. In the United States, prescribing information for all medications licensed for obesity that act on the CNS, including the GLP-1RAs liraglutide 3 mg (Saxenda) and semaglutide 2.4 mg (Wegovy), must include the recommendation of monitoring for depression and suicidal ideation231. This, however, does not apply to other GLP-1RAs approved for the treatment of T2DM, including the same liraglutide (Victoza) and semaglutide (Ozempic or Rybelsus) at lower dosages, prompting several stakeholders to request an updated guidance232 and more caution in media enthusiasm233. Indeed, the history of anti-obesity medications has been marked by several failures due to serious adverse events, such as suicidality, observed only after their usage had become extensive221,234—a well-known example being the one that led to the withdrawal of the endocannabinoid inverse agonist, rimonabant235. Many have advocated that the associations between low mood, suicidal behavior and anti-obesity drugs such as GLP-1RAs are confounded by the pre-existing higher prevalence of neuropsychiatric disorders observed in people living with obesity compared with the general population236. More recently, the European Medicines Agency Pharmacovigilance Risk Assessment Committee concluded that the available evidence does not at present support a causal association between GLP-1RAs and suicidality237. Overall, as GLP-1RAs become increasingly prescribed, further pharmacovigilance studies are warranted.
Second, considering evidence from clinical studies as informed by pre-clinical and mechanistic research, a putative benefit of GLP-1RAs on cognitive disorders (mediated by several neuroprotective mechanisms, especially anti-inflammatory effects; Fig. 1, Table 1, Extended Data Tables 1 and 2, and Supplementary Section 4) and substance-use disorders (via modulation of dopaminergic pathways of reward, impulse control and decision-making; Fig. 1, Table 2 and Supplementary Section 5) seems more likely, while any effect on psychotic, mood and anxiety disorders appears less consistent and in need of further investigation. This would be in line with a recent propensity-score matched cohort study by our laboratory, which observed that semaglutide was associated with reduced cognitive deficit and nicotine misuse when compared against three other antidiabetic medications227. It is also possible that GLP-1RAs may have a therapeutic effect across traditional diagnostic categories. For example, inflammation is known to play a role in at least a subset of depressive238 and psychotic disorders239; therefore, it is conceivable that the use of GLP-1RAs may be beneficial in these patients’ groups—although no studies have specifically assessed these mechanistic aspects in relation to psychopathology in humans thus far. Clinically, GLP-1RAs could lead to an improvement in cognitive function, which is often found to be impaired across several conditions such as psychosis240 and mood disorders241, eventually leading to an overall benefit as observed in some of the included studies (Tables 4 and 5). This notion is speculative at present, as no change in cognition was observed in one small RCT of exenatide in schizophrenia140, while a positive cognitive effect of liraglutide was only seen in an even smaller non-randomized open-label investigation of people with either depressive or bipolar disorders178,179. Notably, an ongoing RCT investigating the effects of semaglutide on pre-treatment cognitive dysfunction in patients with major depression may provide useful insights in this regard (NCT04466345 (ref. 242); Supplementary Section 3).
However, the plausible actions of GLP-1RAs on several reward domains may require more nuanced interpretation. Alcohol- and other substance-use disorders may well benefit from the effects of GLP-1RAs on dopamine and opioid pathways that are dysregulated in addiction243, as seen in some of the studies we identified, and the same could also apply to other under-investigated disorders with similar underlying dysfunctions (for example, gambling disorder). Conversely, people who already present with high anhedonia, for instance, in the context of a depressive illness, may see their symptoms worsening when on GLP-1RAs—which could elucidate some of the studies reporting negative effects associated with these medications in mood and anxiety disorders. As hinted above, this predicament could be disentangled via studies that include a mechanistic assessment of biomarkers predicting response versus harm following GLP-1RA administration192.
Any potential transdiagnostic benefit of GLP-1RAs may be amplified by their established effects on cardiovascular and metabolic morbidity and mortality21,22, which are known to be raised in several cognitive and mental health disorders244,245. Indeed, an important issue for the potential cognitive and mental health effects of GLP-1RAs, which our analysis cannot fully address, is whether these medications provide symptomatic relief only via their well-established cardiometabolic benefits, or by directly targeting physiopathological mechanisms behind cognitive and mental symptoms. Only a minority of studies, that is, four in Parkinson’s disease52,53,54,55, five in substance-use disorders111,113,115,116,117, one in psychotic disorders144 and two in mood disorders178,179,182, assessed the cognitive and mental health effects of GLP-1RAs in non-diabetic, non-obese populations. As research on GLP-1RAs expands in the cognitive and mental health area, we may be able to distinguish between direct effects on cognitive and mental health outcomes and effects that are mediated by GLP-1RAs’ actions on cardiovascular and metabolic outcomes. The numerous ongoing and planned studies reported in Supplementary Section 3 will probably provide more clarity in this regard.
On this note, we also observed a lack of studies examining possible interactions between psychotropic medications and GLP-1RAs—perhaps due to the novelty of the latter. Nevertheless, numerous ongoing trials are investigating the cardiometabolic effects of GLP-1RAs in patients with mental illness, especially for those on antipsychotics (Supplementary Section 3)—such research should therefore address the abovementioned knowledge gap.
Third, we found only a few studies on GLP-1RAs in eating disorders and their psychopathology (Table 6 and Fig. 2). To our knowledge, no study assessed the potential of abuse of these medications anecdotally reported in anorexia or bulimia nervosa, which would require further investigation.
Interestingly, obesity, for whose treatment GLP-1RAs are approved and validated1,214, is not classified under mental and behavioral disorders, and in some countries, such as the United Kingdom, it is not even formally recognized as a disease246. In this context, we note that the remarkable effects of GLP-1RAs in achieving weight loss may fail to be maintained over the long term once medications are stopped247. Some have argued that obesity is a severely under-treated condition, despite its high prevalence, comorbidity with many physical and mental health disorders, and associated mortality and societal cost246. Although several psychological factors (for example, deficit in impulse control) are known to play a major role in the pathophysiology of obesity248, we here raise the issue of disparity in the provision of psychiatric care for the treatment of obesity compared with other eating disorders, which are predominantly treated by psychiatrists, and advocate for the importance of a multidisciplinary, integrated approach to weight management.
Fourth, an important issue that is often raised is whether any GLP-1RAs can indeed penetrate the blood–brain barrier and therefore express any neurobiological activity in the CNS, which would result in cognitive or behavioral changes. Some studies in rodents showed that exendin-4 (ref. 249), liraglutide250 and semaglutide5 did not cross the blood–brain barrier but instead interacted with the brain through the circumventricular organs. However, other investigations have suggested that several GLP-1RAs may cross the blood–brain barrier via passive diffusion251, a GLP-1R-mediated uptake mechanism252 or adsorption transcytosis253, although different compounds may present with variable degrees of brain penetrance254. Overall, the extent to which GLP-1RAs cross the blood–brain barrier remains uncertain in pre-clinical studies4, and further discrepancies are expected in translating these data from animals to humans. In addition, some putative effects of GLP-1RAs on cognitive and mental health symptoms may not require direct activity in the CNS, but rather be mediated by the actions that these medications express in the periphery across immune, endocrine–metabolic and gut–brain axis mechanisms (Fig. 1). Finally, another layer of complexity is added when considering the evidence of a leaky blood–brain barrier across several neuropsychiatric disorders255, which could further increase the brain penetrance of GLP-1RAs administered to people with such illnesses.
Limitations
In this paper, our methodology was systematic in nature (Supplementary Section 1) as we sought to maximize the comprehensiveness of our search while providing a balanced overview of available literature. Limitations of this approach, however, include the lack of quantitative analysis and of a structured assessment of the quality of studies and certainty of evidence, which were beyond the scope of this descriptive work. Furthermore, we did not use operationalized criteria (for example, Diagnostic and Statistical Manual 5th edition) to define the populations of interest because these would not be applicable across animal and human studies, but instead relied on the definitions provided by the individual articles. Finally, sex assigned at birth was not assessed in this review work. These limitations can be more appropriately addressed in future systematic reviews with meta-analyses.
Conclusions
Some have argued that GLP-1RAs have the potential to transform medicine and society as we know it256, which will undoubtedly have a profound impact on psychiatric practice. High costs, as well as tolerability issues, remain considerable barriers to a more wide-ranging prescribing of these drugs1. The pharmaceutical industry is developing newer and potentially cheaper or more effective molecules that target GLP-1 and associated pathways (for example, the so-called dual- and triple-agonists tirzepatide, retatutride and orfoglipon)257,258. The promise of GLP-1RAs could materialize for several cognitive and mental health disorders. Still, caution is required because the adoption of general medical treatments into psychiatry (for example, insulin therapy) has sometimes led to deleterious consequences for patients. Conscious of the importance of all the above, we argue for the need of and inquisitive mechanistic and clinically applied research to inform stakeholders about the potential benefits and harms of GLP-1RAs. This should include a more accurate, scientifically sound and perhaps sober guidance of the communication between the media and the public.
Methods
This analysis did not require ethical approval, and a protocol was not pre-registered. We conducted a search of the literature on 20 November 2023 via Ovid SP of PubMed/MEDLINE, Embase, Cochrane CENTRAL and PsycInfo databases from inception, updated with serial manual searches until 13 July 2024. ClinicalTrials.gov and the World Health Organization portal were also reviewed for ongoing or unpublished studies. The broad search algorithm combined index terms and free-text words for all GLP-1-RAs, with no restriction to study language, design (including both individual studies and their meta-analyses), setting, comparator and outcome of interest to maximize the comprehensiveness of the evidence synthesis. The web-based software, Covidence, for semi-automated text mining, and extensive forward/backward searching were employed to support with de-duplicating and screening of records to include only studies relevant to cognitive and mental health disorders. Two researchers (A.G. and O.D.) independently screened titles and abstracts for relevance, assessed the full texts for eligibility and extracted relevant data; disagreements were discussed with a third author (R.D.G.) and resolved by consensus to data validation. Studies were divided between pre-clinical and mechanistic evidence, and clinical evidence; both were fully described so that the former could support the interpretation of the latter. We used a systematic approach to literature searching and data extraction to increase the transparency of the data reported, but no statistical methods were used with the data collected.
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.

Responses