Early life stress and functional connectivity in antipsychotic-naïve first episode psychosis patients

Introduction
Consistent evidence suggests that early life stress functions as a risk factor for the development of psychosis spectrum disorders1 and can significantly impact clinical disease presentation. Specifically, childhood maltreatment or trauma related to experiences of neglect and physical, emotional, and sexual abuse has been identified as a potential risk factor for psychosis2. Evidence suggests that there is a dose response effect for childhood maltreatment and psychosis, with greater and more severe exposure to childhood maltreatment linked to increased risk of psychosis3. Additionally, childhood maltreatment is observed at higher frequencies among psychosis patients as compared to the general population4. Furthermore, maltreatment among psychosis patients is associated with greater severity of symptoms5,6,7, increased functional impairment8,9, more hospital admissions5,6, increased rates of suicidality10, elevated rates of comorbid disorders11,12,13, and higher rates of treatment non-response14 and dropout7. Given that childhood maltreatment both increases the risk of developing a psychotic disorder and influences the clinical presentation of the disease, investigating the neurobiological correlates of childhood trauma is an important goal to advance scientific knowledge towards early detection and prevention.
The amygdala and hippocampus have bidirectional connections with the ventromedial prefrontal cortex (vmPFC), forming an integrated circuit that mediates emotion expression and regulation processes15. Converging evidence using both structural and functional approaches suggests that interconnections among these regions may be disturbed by stressed-related processes associated with violence exposure or maltreatment during childhood16,17,18,19,20. These findings have been widely demonstrated in the general population21,22,23, and in patients with psychiatric disorders such as major depressive disorder (MDD)24,25 and posttraumatic stress disorder (PTSD)26, but are only starting to garner attention in psychosis. For example, one task-based functional magnetic resonance imaging (fMRI) study reported an association between childhood trauma and changes in hippocampal activity27.
There have only been a handful of fMRI functional connectivity studies involving childhood maltreatment among psychosis patients28,29,30. In a small cohort of schizophrenia patients, Cancel, Comte28 found that childhood trauma subtypes were associated with decreased connectivity between the precuneus/PCC region and amygdala in relation to a negative emotional valence condition. In a recent paper by Dauvermann, Mothersill29, childhood maltreatment in schizophrenia patients was associated with increased pre-frontal cerebellar resting state functional connectivity. Functional impairments of these brain regions can lead to affective functioning deficits, which are considered to be a principal feature of psychosis spectrum disorders31. Furthermore, disruptions of the connections between these brain regions can impair processing of emotion and lead to misinterpretation of interpersonal communication—critical mechanisms underlying the development of psychosis32. The objective of the current study is to expand on this growing area of research and examine the relationship between childhood trauma and functional connectivity between fronto-limbic regions during resting state functional magnetic resonance imaging (rs-fMRI) in antipsychotic-naïve patients with first-episode psychosis (FEP) and healthy controls (HC) in a large sample. We predict that childhood maltreatment will be associated with fronto-limbic alterations.
Results
Demographic data are summarized in Table 1. Patients did not differ from HC on age, sex, or parental occupation; however, they did differ on smoking and education, with healthy controls smoking more packs per day (t(108.146) = −5.677, p <0.001) and having higher education (t(172) = 7.231, p < 0.001). There were also significantly less cannabis users in the healthy control group (t(115.488) = −10.704, p < 0.001). In terms of race/ethnicity, chi-square tests with post hoc analyses examining adjusted residuals indicated that there were more Black participants in the FEP group, more Asian and White individuals in the HC group, and no significant group differences with the Latino/Hispanic or Other race/ethnicity categories (χ2 (4) = 36.01, p < 0.001). For FEP patients, mean total BPRS was 47.46 and mean duration of untreated psychosis was 21.39 months.
Independent samples t-tests comparing mean CTQ total and subscale scores between FEP patients and HC indicated that patients had significantly higher CTQ total (t(90.25) = −4.61, p < 0.001, two-sided) scores. Additionally, FEP patients had significantly higher physical abuse (t(96.31) = −2.88, p = 0.002, two-sided), emotional abuse (t(105.97) = −4.06, p < 0.001, two-sided), sexual abuse (t(83.47 = −4.17, p < 0.001, two-sided), physical neglect (t(90.24 = −3.64, p < 0.001, two-sided), and emotional neglect (t(101.68) = −2.98, p = 0.004, two-sided) subscale scores (see Fig. 1).

Violin plots of CTQ scores illustrating differences between FEP patients and HC where each dot corresponds to one participant. FEP patients had significantly higher scores on all subscales and overall total. FEP first episode psychosis, HC healthy control; ** p < 0.01; *** p < 0.001.
One-way ANCOVA analyses examining rs-FC group differences while controlling for age, sex, and motion (see Fig. 2) indicated that FEP patients had significantly reduced rsFC compared to HC in left amygdala – vmPFC (F(1, 223) = 8.73, p = 0.003, 95% CI [−0.10, −0.02]), right amygdala – vmFC (F(1, 223) = 13.66, p < 0.001, 95% CI [0.58, 0.13]), left hippocampus – vmPFC (F(1, 223) = 4.97, p = 0.027, 95% CI [0.31, 0.38]), and right hippocampus – vmPFC (F(1, 223) = 4.74, p = 0.030, 95% CI [0.28, 0.35]).
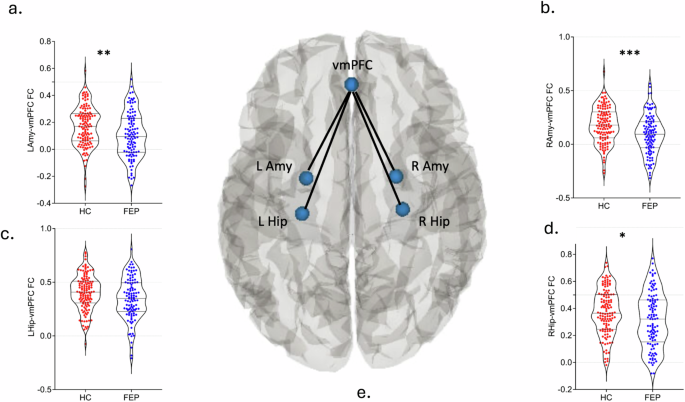
Violin plots of rs-FC illustrating group differences between FEP patients and HC while controlling for age, sex, and motion. FEP patients had significantly reduced rsFC compared to HC in a left amygdala – vmPFC, b right amygdala – vmFC, c left hippocampus – vmPFC, and d right hippocampus – vmPFC. e Visual representation of the pairwise connections between our ROIs. Lamy left amygdala, RAmy right amygdala, LHip left hippocampus, RHip right hippocampus, vmPFC ventromedial prefrontal cortex, FC functional connectivity; * p < 0.05; ** p < 0.01; *** p < 0.001.
Partial correlation analyses for patients are depicted in Table 2. Results indicated that higher CTQ sexual abuse subscale scores in patients were associated with increased left amygdala – vmPFC rsFC (r(59) = 0.27, p < 0.05) and higher CTQ emotional neglect subscale scores in patients were also associated with increased left hippocampus – vmPFC rsFC (r(59) = 0.26, p < 0.05). All other partial correlation analyses were not significant.
Linear regression analyses showed that the overall model significantly predicted left amygdala – vmPFC rsFC (F(6, 153) = 2.77, p = 0.014, R2 = 0.313), with the model explaining 31.3% of the variance in left amygdala – vmPFC rsFC. The interaction between group status and the CTQ sexual abuse subscale was statistically significant (({rm{beta }}) = 0.52, p = 0.037). Simple slopes analyses showed that higher CTQ sexual abuse subscale scores were associated with increased left amygdala – vmPFC rsFC in the FEP patient group (({rm{beta }}) = 0.56, p < 0.001) but reduced rsFC in the HC (({rm{beta }}) = −0.56, p < 0.001) group (see Fig. 3). The interaction between group and the CTQ emotional neglect subscale was not significant.
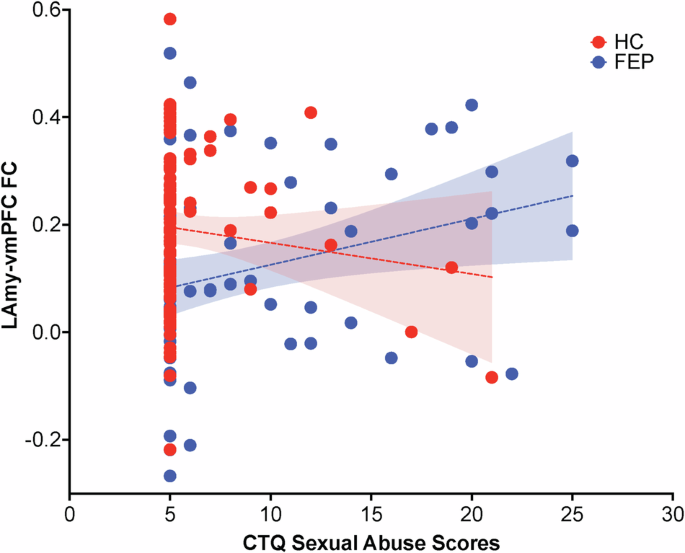
Interaction plot illustrating the relationship between group and CTQ sexual abuse subscale scores on left amygdala – vmPFC functional connectivity. The red line represents the HC group, and the blue line represents the FEP group. The x-axis represents the CTQ sexual abuse subscale, while the y-axis shows mean left amygdala – vmPFC FC. Functional connectivity between the left amygdala and vmPFC was negatively correlated with CTQ sexual abuse subscale scores in healthy controls and positively correlated with CTQ sexual abuse subscale scores in patients. CTQ Childhood Trauma Questionnaire, FEP first episode psychosis, HC healthy controls, Lamy left amygdala, FC functional connectivity, vmPFC ventromedial prefrontal cortex.
As a supplemental analysis, independent samples t-tests were also conducted to compare mean CTQ total subscale scores between the two largest racial/ethnic groups in the sample (Black and White individuals). Within the healthy control group, Black participants endorsed significantly greater physical abuse (8.35 (pm) 2.69) (t(68) = −2.124, p = 0.037) and sexual abuse (7.74(pm) 4.892) (t(23.469) = −2.369, p = 0.026) scores, as compared to White participants. Within the FEP group, there were no significant differences in CTQ total, or subscales scores based on these two racial categories.
Discussion
The current study sought to further elucidate the neurological impact caused by childhood trauma on psychosis patients. Overall, the results indicated that compared to HC, the FEP group had significantly higher CTQ subscale and total scores and reduced rsFC in in the fronto-limbic regions of interest. FEP patients also showed a positive relationship between two of the subscale scores and rsFC of the right amygdala and left hippocampus. Interestingly, follow-up analyses also revealed a significant effect of group on the relationship between the CTQ sexual abuse subscale and left amygdala –vmPFC rsFC, with patients showing increased rsFC as scores on this subscale increased, while HC showed decreasing rsFC as scores on this subscale increased. Additionally, we chose to examine race/ethnicity differences in childhood maltreatment because participants from ethnic minority groups are disproportionately affected by both childhood maltreatment and psychosis33,34. Interestingly, we did not find significant differences in childhood maltreatment based on race within the FEP group.
Supporting the literature on the negative effects of childhood maltreatment on limbic region FC26,30,35,36, initial group-level analysis results indicated that exposure to sexual abuse was associated with significantly decreased left amygdala – vmPFC rsFC in HC. Correlations between amygdala –medial prefrontal regions are typically negative at rest37, which reflects top-down regulatory control38. These results suggest that the healthy controls are exhibiting intact top-down regulatory control via fronto-amygdala neurocircuitry, despite exposure to early life stress38.
In line with previous studies that examined trauma and brain functioning39,40, our FEP patient-specific findings showed that compared to HC, patients had significantly reduced rsFC in all regions of interest. These results highlight that there are distinct patterns of amygdala-prefrontal connectivity that distinguish patients with psychosis from HC. Interestingly, when childhood maltreatment was included in the statistical model as a continuous variable, our patient-specific findings showed increased left amygdala – vmPFC FC. It would be expected that amygdala-vmPFC connectivity would be lower in trauma exposed FEP patients given the additive effects of trauma and psychosis. However, our finding of hyperconnectivity between the vmPFC and amygdala in FEP patients in relation to childhood sexual abuse supports other work which has demonstrated increased medial PFC activity patterns in the dissociative subtype of PTSD41,42. These studies suggest that trauma-related neural adaptations are not uniform but vary based on the type and timing of the trauma. Additionally, hyperconnectivity between amygdala and vmPFC is well documented in rodent models of social defeat in the setting of depleted serotonin and is thought to be a marker of vulnerability43,44,45. Child abuse has been linked to increased chromatin methylation of genes related to serotonin regulation46,47,48. Serotonin regulatory genetic polymorphisms have been associated with risk of later development of psychiatric disorders in people who have experienced abuse as children49,50. The Social Defeat hypothesis for psychosis was postulated by Selten and Cantor-Graae observing neurobiological similarities between defeated animals in the resident intruder paradigm and patients with psychosis51,52. Taken together, hyperconnectivity between amygdala and vmPFC in patients with psychosis and childhood sexual abuse would be predicted within the social defeat hypothesis framework. Thus, these results provide indirect support for the social defeat hypothesis.
In line with the approach Souza-Quiroz (2016), we chose to restrict our ROIs to the amygdala, hippocampus, and ventromedial prefrontal cortex because these regions are consistently identified as key circuits impacted by childhood maltreatment30,19 and implicated in the development of psychosis. However, childhood maltreatment is associated with disruption to other areas of the brain, including sensory neurocircuitry53 and the cingulate cortex54, among other regions. Upstream regions, such as the primary sensory cortices or thalamus, could contribute to differentiating FEP from controls. However, upstream changes alone are not often enough to fully explain or address the long-term sequelae that arise from childhood maltreatment. Alterations in downstream brain areas in the current study provide a more comprehensive picture of how childhood maltreatment experiences shape cognitive, emotional, and behavioral functioning. Additionally, the cingulate cortex is functionally diverse, with involvement related to emotion regulation, self-referential processing, memory processes, and attention, among other functions55. While relevant, trauma-related changes to the cingulate cortex are not as well documented in the psychosis literature and may be secondary in the trauma-psychosis pathway, compared to the hippocampus-amygdala-ventromedial prefrontal cortex circuit. However, future investigations incorporating a broader range of regions may help elucidate the mechanisms behind the complex interplay between exposure to childhood maltreatment and functional connectivity.
This study has several strengths and limitations. Our sample size was large and consisted of medication-naïve patients with first episode psychosis. Since the majority of the patient sample had no prior exposure to antipsychotic medications prior to the scan, we had the opportunity to conduct this study with minimal concerns related to possible confounds from medication exposure. We also chose to analyze the subscales of the CTQ, which allowed us more nuanced insights into how different trauma subtypes can differentially impact neurobiology. However, evidence suggests that severity and timing of trauma can differentially impact limbic regions56, but the CTQ does not account for age of onset, duration of maltreatment, or timing of the event. Additionally, as a retrospective self-report measure, the CTQ may be vulnerable to reporting bias.
Our findings show evidence that the impact of childhood trauma on brain mechanism patterns differ significantly between the general population and individuals with psychosis spectrum disorders. The results also provide support for the lasting differential influence of trauma subtypes on the brain. The findings show that psychosis patients with a history of childhood maltreatment form a distinct group characterized by unique neurobiological correlates. Overall, the results contribute to the understanding of the neural mechanisms underlying the association between childhood trauma and psychosis spectrum disorders.
Methods
Participants
One hundred and fifteen first-episode antipsychotic- naïve psychosis patients were recruited from the emergency department, outpatient clinics, and inpatient services within the Department of Psychiatry at the University of Alabama at Birmingham. Approval was obtained from the ethics committee of University of Alabama at Birmingham and written informed consent was obtained from all individual participants included in the study.
One hundred and twenty-six HC were recruited from the surrounding community. Exclusion criteria included major medical conditions, diagnosable central nervous system illnesses, pregnancy, major medical conditions (e.g., seizure disorders, traumatic brain injury, brain tumors, cephalic disorders, stroke, etc.), history of head trauma, active substance use (with the exception of nicotine and cannabis), and MRI contraindications. Participants with a history (less than a year) of substance (with the exception of nicotine and cannabis use) or alcohol abuse were also excluded. There were 241 recruited participants and 13 were excluded after quality control (see data reprocessing), leaving us with a total sample size of 228 (FEP = 105, HC = 123).
Clinical assessment
Psychiatric diagnoses were made in consensus following DSM-5 criteria by two board-certified psychiatrists using all available historical information and direct assessment. Participants were given the Childhood Trauma Questionnaire (CTQ) to assess for adverse childhood events57. The CTQ is a retrospective questionnaire which produces five subscales: physical abuse, emotional abuse, sexual abuse, physical neglect, and emotional neglect. The short version (28 items) of the CTQ was utilized for the current study. To ensure the accuracy of all information provided, the current study used information from all available collateral informants.
Data acquisition
Imaging was performed with a 3 T whole-body Siemens MAGNETOM Prisma MRI scanner (Siemens, AG, Erlangen, Germany) equipped with a 20-channel head coil. A T1-weighted structural scan was acquired (magnetization prepared rapid acquisition gradient-echo: repetition time = 2400 ms; echo time = 2.22 ms; inversion time = 1000 ms; flip angle = 8 degrees; generalized autocalibrating partially parallel acquisitions [GRAPPA] factor = 2; voxel size = 0.8 mm3). Resting state functional MRI data were obtained in opposing phase encoding directions (anterior > posterior and posterior > anterior; repetition time = 1550 ms; echo time = 37.80 ms; flip angle = 71 degrees, field of view = 104 mm2; multiband acceleration factor = 4; voxel size = 2 mm3; 225 volumes, and 72 axial slices). The first 10 volumes on each fMRI run were discarded in order to allow for signal equilibration. Susceptibility artifacts were corrected via spin echo field maps in FSL’s topup and the two corrected fMRI runs were concatenated, resulting in a single 4-dimensional image of 430 volumes total. All participants underwent a resting state fMRI scan that lasted approximately 12 min. They were instructed to keep their eyes open and stare passively ahead.
Data preprocessing
Data preprocessing was conducted in CONN functional connectivity toolbox version 20.b58. Preprocessing consisted of motion correction and slice-timing, coregistration to the structural image, low-bandpass filtering (0.008 < f < 0.08 HZ), normalization to the Montreal Neurological Institute (MNI) space, and spatial smoothing with a 4-mm full width at half maximum Gaussian kernel.
Percentage of censored data and framewise displacement were calculated. Using the Artifact Detection Tools toolbox (NeuroImaging Tools and Resources Collaboratory), motion outliers were detected and then censored (composite volume to volume motion >0.5 mm and intensity >3 SDs). First component time series derived from white matter and CSF masks using aCompCor within the CONN toolbox and corresponding derivatives, as well as six motion parameters derived from rigid-body realignment and their derivatives were regressed out from the signal. In summary, FC datasets from 105 FEP and 123 HC were included in the final analyses (10 FEP patients and 3 HC were excluded from the total recruited sample).
Statistical analyses
Regions of interest (ROI) were defined using the FSL Harvard-Oxford Atlas within CONN and included bilateral hippocampi, amygdalae, and vmPFC. For fronto-limbic rs-FC analyses, FC was calculated using the conn_withinbetweenROItest function implemented in CONN by averaging the BOLD signal across a set number of ROIs. This computes Pearson’s correlation across those ROIs and then creates an average within and between FC value. For each subject, we computed the following pairwise connections: right amygdala – vmPFC, left amygdala – vmPFC, right hippocampus – vmPFC, and left hippocampus – vmPFC. These FC values were then z-transformed. We did not compute amygdala-hippocampus connectivity.
Independent samples t-test were performed to examine group differences between FEP patients and HC on CTQ total and subscale scores. Analysis of variance (ANCOVA) tests were conducted to examine group differences in fronto-limbic rsFC while controlling for age, sex, and framewise displacement. A Bonferroni correction was applied to adjust for multiple comparisons in the ANCOVA analyses. Partial correlation analyses controlling for age, sex, and framewise displacement were conducted separately for FEP patients and HC to examine the relationship between CTQ total and subscale scores and fronto-limbic rsFC. Multiple linear regression analyses were performed to examine the moderating role of group in the relationship between fronto-limbic rsFC and the CTQ subscale scores. Age, sex, and framewise displacement were included in the models as covariates as well. Significant interactions were then followed by simple slopes analyses for HC and FEP patients. All p-values reported are two-sided.



Responses