Reconceptualizing menstrual health and hygiene among young women in India

Introduction
For millions of individuals who menstruate in India, managing menstrual needs is a significant challenge, exacerbated by especially in the context of resource constraints common to low-and-middle-income countries1. Ensuring dignified menstrual management is essential for their well-being and participation in daily life2. This is not simply a matter of personal hygiene but a critical public health and human rights issue3, central to gender equality and social justice. Addressing this issue, is fundamental to achieving the Sustainable Development Goals (SDGs)4, as improving MHH contributes to progress across the entire 2030 Agenda for Sustainable Development5.
While awareness of MHH is increasing, research and public health agendas have often focused narrowly on individual components, such as the affordability and access to period products, or access to sanitation facilities6. However, a more comprehensive understanding of MHH is emerging, recognizing it as a multifaceted issue encompassing sociocultural support, menstrual knowledge, and safe practices5,7,8. Crucially, a significant gap remains in understanding how these factors interact and their combined influence on overall MHH adequacy. To address this gap, robust measures capturing the interconnectedness of these concepts are essential. While the definition of MHH continues to evolve, the need for integrated assessments remains crucial9,10.
This study uses the core definition of good MHH put forth by WHO & UNICEF Joint Monitoring Program, which is defined as: “using a clean menstrual management material to absorb or collect menstrual blood, that can be changed in privacy as often as necessary for the duration of a menstrual period, using soap and water for washing the body as required, and having access to facilities to dispose of used menstrual management materials11.
Indian studies on MHH have primarily focused on the usage of period products and associated socioeconomic, biodemographic, women-empowerment, and mass-media-related factors4,12,13,14,15,16,17 While valuable, these studies often examine period product usage and water, sanitation, and hygiene (WASH) access separately, limiting our understanding of their combined influence on MHH adequacy. Addressing menstrual health goes beyond simply providing period products; it necessitates creating enabling environments that allow individuals to manage menstruation with dignity and comfort18. This includes addressing the pervasive issue of period poverty, characterized by limited access to affordable and safe period products and inadequate facilities for private menstrual management.
Responses to public interest litigation, including directives from the Supreme Court, emphasized the urgent need for a unified national policy on menstrual health, which should guarantee free access to both period products and adequate toilet facilities. Such legal interventions highlight the growing recognition of menstrual health as a critical public health issue in India. In response to these developments, Babbar & colleagues introduced the novel MHH Index, which integrates key indicators such as period product usage and access to improved sanitation facilities19. This index marked a significant step toward understanding and addressing disparities in menstrual health across regions. This integrated perspective is essential for developing comprehensive and effective interventions. Our study addresses this gap by examining both period product use and WASH access within a holistic MHH framework. Our study builds on this crucial work by further expanding the MHH Index to incorporate comprehensive WASH facilities.
To address the identified research gaps and contribute to a more holistic understanding of MHH, our study has three key objectives:
-
a.
Refine the conceptualization of MHH by integrating period product usage and WASH facilities as essential components. This integrated approach will provide a more complete and accurate assessment of MHH adequacy.
-
b.
Assess the prevalence of adequate MHH, using this integrated framework, among girls and women across various socioeconomic groups in India, analyzing the variations in access across different population segments. This will reveal the magnitude of the challenge and identify populations most in need of interventions.
-
c.
Analyze the geographical distribution of adequate MHH at the district level, examining the significant predictors associated with it and identifying factors contributing to the gap between the top 25% high-performing and the bottom 25% poor-performing districts. This spatially nuanced analysis will offer critical insights for developing geographically targeted interventions.
By comprehensively understanding these disparities and their underlying factors, our study aims to inform the development of targeted interventions and policies that can effectively address the multifaceted nature of MHH and promote menstrual equity across the country.
Results
Profile of the respondents
Table 1 presents the background characteristics of 205,861 sampled women aged 15–24 years included in this study. The majority (64.3%) had never been married and most resided in rural areas (70.7%). Over two-thirds (67.9%) had attained secondary education, and an additional 19.4% higher education. The sample was largely Hindus (82.5%), followed by Muslims (13.4%) and Christians (1.8%). Socially, the largest proportion belonged to the Other Backward Classes (46.1%), while Scheduled Castes and Other categories represented 24.3% and 20%, respectively. In terms of wealth, the richest category represented 20.2% of the sample. As for media exposure, 41.5% of sampled women read newspapers, 14.4% listened to the radio, and 75.3% watched television. Furthermore, a significant proportion reported various barriers to accessing healthcare: obtaining permission to seek medical help (39.1%), obtaining money for treatment (50.9%), distance to health facilities (57.3%), and transportation challenges (55.1%).
Status of different components of MHH among girls and women aged 15–24 years in India, NFHS-5 (2019–21)
In India 78.6% women aged 15–24 years had access to water within premises, and 74.3% had soap available at the handwashing point. While nearly half (49.5%) reported using period products during menstruation, only 27.7% had access to all four essential MHH resources including using appropriate period products, an improved unshared toilet, water within the premises, and soap at the handwashing point. This indicates that a large majority of young women in India lack access to adequate MHH resources.
Adequate MHH by background characteristics among young women, NFHS-5 (2019–21)
Table 2 shows the prevalence of adequate MHH across background characteristics, revealing significant differences in access. Age at menarche showed a small positive association, with women experiencing menarche at 16 years or older having a slightly higher prevalence (31.4%) compared to those with menarche at age 12 or younger (28.4%). Marital status was strongly associated with adequate MHH; widowed, divorced, or separated women had the lowest prevalence (13.1%), followed by married women (21.5%), while never-married women had the highest prevalence (31.5%).
Education level demonstrated a significant role, with prevalence ranging from 5.4% among women with no formal education to 47.4% among those with higher education. Religion affiliation was also significant, with Christian women (38.3%) and women of other religions (50.8%) exhibiting higher prevalence than Hindu (27.2%) or Muslim (26.7%) women.
We observed significant differences across social groups, with women in the “Other” category having the highest prevalence (41.5%), followed by Other Backward Classes (27.6%), Scheduled Tribes (14.7%), and Scheduled Castes (22.3%). In the NFHS-5, the “Other” category within the social group classification refers to individuals who are not included in the three socioeconomically and historically marginalized groups officially designated by the Government of India: Scheduled Castes, Scheduled Tribes, and Other Backward Classes. “Other” is thus a residual category and it predominantly comprises individuals from caste groups occupying the upper levels of the caste-based social hierarchy. Wealth status, as measured by the asset index, was strongly and positively associated with adequate MHH, ranging from 4.7% for women from the poorest category to 59.0% among the richest. Place of residence revealed a substantial gap, with urban women (48%) having a much higher prevalence than rural women (19.4%).
Regional disparities were also evident, with the North (44.8%) and West (40.3%) showing higher prevalence than other regions. Media exposure was positively associated with adequate MHH, while barriers to healthcare access (permission, financial, distance, transportation) were associated with lower prevalence.
Geographical disparities in adequate MHH across the Indian districts
Figure 1 highlights substantial district-level variations in access to adequate MHH across India, ranging from 2.3% in the Karimganj district (Assam) to 89.4% in the Champhai district (Mizoram). 25% of districts had very low prevalence rates (below 16%), concentrated primarily in the states of Uttar Pradesh (31), Madhya Pradesh (18), Odisha (18), Jharkhand (16), Chhattisgarh (14), Assam (11), and parts of Karnataka (7) and West Bengal (6).

District-wise access to adequate MHH in India, NFHS-5, 2019–21.
Determinants of adequate MHH among girls and women aged 15–24 years in India, NFHS-5 (2019–21)
Table 3 presents the odds ratio (OR) and 95% confidence interval (CI) from multivariate logistic regression. Several factors were significantly associated with the odds of having access to adequate MHH. Compared to never-married women, currently married women had significantly lower odds (AOR: 0.82, 95% CI: 0.79, 0.85). Education level showed a strong positive association, with each increase in education level associated with progressively higher odds of adequate MHH. Women with higher education had over three times the odds of adequate access (AOR: 3.23, 95% CI: 2.89, 3.60) compared to women with no formal education. Similarly, wealth as measured by the asset index, demonstrated a strong positive gradient. Women in the richest quintile had nearly ten times the odds of adequate MHH (AOR: 9.92, 95% CI: 9.11, 10.81), compared to those in the poorest quintile.
Religious affiliation, social group, place of residence, and region of residence also showed significant associations. Muslim women (AOR: 0.87, 95% CI: 0.83, 0.92), Scheduled Castes (AOR: 0.71, 95% CI: 0.68, 0.75), Scheduled Tribes (AOR: 0.61, 95% CI: 0.57, 0.65), and Other Backward Classes (AOR: 0.82, 95% CI: 0.79, 0.85) all had lower odds of adequate MHH compared to Hindu women and the “Other” social group, respectively. Regionally, women in the Northern and Western regions had approximately twice the odds of adequate access compared to those in the Central region.
Place of residence played a significant role in adequate MHH, as urban women had higher odds of practicing adequate MHH (AOR: 1.97, 95% CI: 1.90, 2.04) compared to rural women. The region of residence was also associated with varying odds of adequate MHH.
Media exposure, specifically reading newspapers (AOR: 1.45, 95% CI: 1.38,1.52) at least once a week, was positively associated with adequate MHH. Among the barriers to accessing medical help, financial constraints (AOR: 0.78, 95% CI: 0.75, 0.82), distance to health facilities (AOR: 0.93, 95% CI: 0.89, 0.97), and transportation issues (AOR: 0.89, 95% CI: 0.85, 0.93) were all significantly associated with lower odds of adequate MHH.
Results of Fairlie decomposition analysis
We conducted a Fairlie decomposition analysis to quantify the predictors contributing to the disparity in adequate MHH access between the top and bottom quartile of districts. The mean predicted probabilities of adequate access for the bottom and top quartiles were 0.53 and 0.11, respectively, indicating a substantial gap of 0.42.
Our analysis revealed that 72.8% of this gap was explained by the predictors included in our model. Of this explained portion, 76.4% was attributable to differences in the distribution of just three predictors: asset index, area of residence, and region of residence. These findings highlight the crucial role of sociodemographic and geographic factors in shaping disparities in adequate MHH access. However, approximately 27% of the gap remained unexplained by our model, suggesting the potential influence of unmeasured factors not captured in the National Family Health Survey (NFHS)-5 data. These unmeasured factors could include individual-level factors like knowledge and attitudes related to MHH, community-level factors such as social norms and stigma, and programmatic factors like the availability and quality of MHH interventions.
Table 4 provides a more detailed breakdown of decomposition results, expressing each predictor’s contribution as a percentage of the explained gap. The asset index emerged as the most significant contributor, accounting for 36.5% of the explained disparity between high- and low-performing districts. Region of residence (23.6%) and place of residence (16.7%) were the next most influential factors. Education level and exposure to reading newspapers also made notable contributions (6.3% and 4.7%, respectively).
Discussion
Achieving universal access to safe and hygienic MHH is crucial for individual empowerment, gender equity, and overall public health in India, and the government, grassroots innovators, academicians, and policymakers are doing their best to achieve it. This is a multifaceted challenge influenced by a complex interplay of factors, with access to both appropriate period products and adequate WASH infrastructure being fundamental. Past literature has argued that the core concepts defining MHH remain consistent8. Our study builds upon previous research, and the MHH index19 and empirically testing the WHO & UNICEF (2012) Joint Monitoring Program11.
This study makes several key contributions. First, we reconceptualize MHH by expanding its scope beyond period product usage to include WASH facilities, leading to a more holistic understanding. This integrated approach offers a more nuanced understanding of MHH adequacy. Second, by analyzing district-level variations, we provide geographically granular insights into MHH disparities. Third, we contribute to the growing literature on gender and public health in India. Overall, our findings, combined with the existing research, offer a roadmap for targeted policy and program development in India.
This study has several strengths. First, it utilizes a nationally representative dataset (NFHS-5), allowing for generalizable conclusions about MHH access among young women in India. Second, it advances MHH research by integrating WASH facilities alongside period product utilization, offering a more holistic and nuanced understanding of MHH adequacy. Third, the district-level geographical analysis provides valuable insights into the spatial distribution of MHH access, highlighting critical regional disparities and the need for place-based interventions. Finally, the use of Fairlie decomposition allows for a quantitative assessment of the factors driving disparities, providing actionable evidence for policy development.
Our analysis reveals that that only 27% of young women have access to adequate MHH infrastructure, highlighting the urgent need for action. The substantial differences across districts, ranging from less than 4% (Karimganj and South Salmara Mancachar in Assam), to over 80% (Kolasib, Serchhip, Aizawl, and Champhai in Mizoram) access, underscore the inequitable distribution of resources and opportunities. These significant disparities prompted the next phase of our study, in which we classified districts into two groups—the top 25% with higher MHH prevalence and the bottom 25%. By analyzing the factors contributing to this gap, we identify key areas for intervention.
Socioeconomic factors, majorly asset index (36%), emerged as the strongest predictor of adequate MHH. The disparity between the poorest (4% with access) and the richest (59% with access), reveals the stark realities of period poverty, encompassing both financial constraints in accessing products and limited access to basic WASH amenities. This highlights the need for a two-pronged approach. While ensuring free or subsidized products is crucial, it is insufficient without concurrent investment in WASH infrastructure. Access to WASH is not merely a supporting factor but a core component of adequate MHH. This includes constructing and maintaining safe, private toilets, ensuring reliable water sources specifically designated for menstrual hygiene management, and providing accessible handwashing stations with soap and water. Promoting affordable and reusable options, like reusable pads and menstrual cups, can further alleviate the financial burden, but access to WASH remains essential for their hygienic use17.
Regional and area of residence disparities contribute significantly (40%) to the MHH gap. This disparity is particularly evident in WASH access. Lower access in the central, eastern, and northeastern regions compared to north, south, and west17,20,21, likely reflects variations in socioeconomic development, healthcare infrastructure, and policy implementation. This demands regionally tailored strategies, focusing on WASH improvements in underserved areas. Improving WASH in these regions must be prioritized. For instance, regions with low toilet coverage could prioritize school toilet construction and community sanitation programs. Areas with limited water access require investment in water supply infrastructure dedicated to MHH needs.
Education and mass media exposure contribute to greater MHH access, highlighting the importance of empowering women with knowledge and challenging harmful social norms. Education improves earning potential and enhancing their bargaining power within the household17,22. It also reduces shame and stigma23,24, enabling informed choices. Mass media can disseminate MHH information and challenge traditional beliefs & taboos, especially in rural areas25,26,27.
Based on our findings, we recommend that targeted interventions must integrate WASH components, including (a) conditional cash transfers linked to household WASH improvements; (b) school-based programs providing MHH education, products, and functional WASH facilities; (c) community-led initiatives promoting WASH construction and maintenance; (d) public-private partnerships to improve product and WASH infrastructure access; and (e) mass media campaigns promoting both product use and hygiene practices reliant on adequate WASH.
Future research should explore the (a) impact of specific WASH interventions on MHH; (b) lived experiences of women, particularly regarding WASH challenges; and (c) culturally tailored WASH solutions. Our study is limited by the NFHS-5 age range (15–24 years) and lack of data on specific MHH practices and transgender/non-binary individuals28.
Our study reinforces the importance of integrating period product usage and WASH facilities as essential components of adequate MHH. It highlights the need for targeted interventions and policies to address disparities in MHH access across different socioeconomic groups, regions, and areas of residence. Empowering individuals through education, promoting affordable alternatives, and leveraging mass media are crucial steps toward achieving universal access to safe and hygienic menstrual management in India.
Methods
Data source
This study uses data from the nationally representative NFHS-5 conducted in India from 2019–21. The NFHS-5 employs a multi-stage stratified cluster sampling design to collect information on various health and development indicators, including sexual and reproductive health, perinatal mortality, and non-communicable diseases. Firstly, primary sampling units (PSUs) were selected, followed by households within each PSU, and finally, eligible women aged 15–49 within selected households. The survey gathered information from 636,699 households and 724,115 women aged 15–49 across India’s 28 states, 8 union territories, and 707 districts. While the NFHS-5 collected data from women aged 15–49, information on period product usage—a key variable for our study—was only available for women aged 15–24 years. Therefore, our analysis focuses on this age group.
To construct our analytical sample, we merged individual and household-level data files from the NFHS-5 for women aged 15–24 years who responded to questions about period product usage i.e., 241,180. After excluding cases with missing data, our final analytical sample consisted of 205,861 women (see Fig. 2 for details).
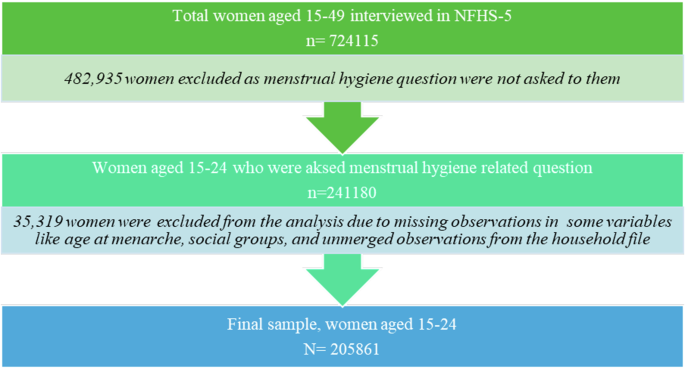
Process of analyzed sample size selection from the NFHS-5 dataset.
Outcome variable
Our primary outcome variable is “adequate MHH”. To operationalize this concept, we initially considered six key variables using NFHS-5 data: use of period products during menstruation, taking bath in the bathroom during menstruation, availability of water within the premises, daily availability of water, availability of improved unshared toilets within the premises, availability of soap at the handwashing point. We then conducted a principal component analysis (PCA) to construct a reliable and valid measure of adequate MHH.
PCA was conducted on six initial variables related to MHH. The analysis revealed three components with eigenvalues greater than one (see Supplementary Table 1 and Supplementary Fig. 1 for the six-component PCA). Based on the loadings of each variable, conceptual considerations, and a secondary PCA with four components, we retained a single principal component that explained 37% of the variance. This component was strongly associated with four key variables: use of modern period products (loading = 0.42), availability of water within the premises (loading = 0.48), availability of an improved, unshared toilet (loading = 0.56), and availability of soap at the handwashing point (loading = 0.53). The excluded variables from the initial six, “taking a bath in the bathroom” and “daily water availability,” loaded less strongly on this primary component (see Supplementary Table 2 and Supplementary Fig. 2) and were considered less directly related to the core elements of adequate MHH as defined by WHO/UNICEF, which emphasizes access to clean menstrual materials, soap and water for washing, and private facilities for managing menses. This four-variable indicator thus aligns strongly with established definitions of adequate MHH.
Use of period products during menstruation
The NFHS-5 asked respondents about materials they used during their menstrual cycles to manage blood flow. For this study, this variable was dichotomized to indicate exclusive use of modern period products (sanitary napkins, tampons, menstrual cups). Respondents who reported using only modern products were coded as 1, while those who reported using cloth, no products, or any combination of modern and non-modern methods were coded as 0. This aligns with the methodological approach used in previous studies16,29,30.
Water within premises
This variable indicates the availability of piped drinking water within the respondent’s dwelling or yard/plot, coded as 1 for access, and 0 for no access20.
Improved toilet within premises
This variable was coded as 1 if the household had access to improved toilet facilities (flush/pour flush toilets connected to piped sewer systems, septic tanks, or pit latrines with a slab, as well as ventilated improved pit (VIP)/biogas latrines and twin pit/composting toilets) within the premises that were not shared with other households. If the toilet facility was not considered “improved” or was shared, the variable was coded as 031,32.
Availability of soap at handwashing points
his variable indicates whether a handwashing facility with soap present was available on the premises. Coded as 1 for available and 0 for unavailable20,31.
Independent variables
Informed by the review of prior research available on MHH in India14,16,17,25,29,30,33,34,35,36, this study includes the following independent variables i.e., age at menarche (in years), marital status, education level of respondents, religion, social group, household asset index, place of residence, region of residence, reading newspaper, listening to radio, watching television, problems of receiving permission to seek medical help, getting money for treatment, distance to health facility and taking transportation. Detailed descriptions and categorizations of each independent variable are provided in Supplementary Table 3.
Statistical analysis
We began by conducting bivariate analysis techniques to explore the differences in access to adequate MHH across various background characteristics. We then used chi-square tests to examine whether significant differences in MHH access existed across the categories of our independent variables.
To identify statistically significant predictors of access to adequate MHH, we then used multivariate binary logistic regression, examining associations between the dependent (adequate MHH) and our set of independent variables. Results are presented as estimated ORs with 95% CIs. We assessed for multicollinearity among independent variables prior to regression analysis to ensure that they were not highly correlated with each other (See Supplementary Table 4).
To visualize geographical patterns, we created a choropleth map using ArcGIS, illustrating the district-level variations in the prevalence of adequate MHH. Based on these prevalence rates, we classified districts into two categories: the top 25% as high-performing districts and the bottom 25% as poor-performing districts.
To quantify the factors contributing to the gap in adequate MHH between these high-performing and poor-performing districts, we employ Fairlie decomposition analysis, using the ‘fairlie’ package available in Stata 16. This technique allows us to decompose the difference in mean predicted probabilities of adequate MHH access into the portions attributable to each predictor variable included in the logistic regression model. This decomposition helps identify the key drivers of inequality and provides valuable insights for targeted interventions aimed at reducing disparities. All analyses accounted for the complex survey design of the NFHS-5 using appropriate sampling weights and the “svyset” command in Stata.
Ethical approval
Ethical approval for NFHS-5 (2019–21) was provided by the International Institute for Population Sciences (IIPS), Mumbai, and further reviewed and approved by the ICF International Review Board to ensure compliance with ethical guidelines. Participants were fully briefed about the objectives and procedures of the survey, and written consent was obtained before conducting any interviews. Participation was entirely voluntary, and interviews were only carried out after obtaining informed consent. The data used for this study are publicly accessible via the Demographic and Health Surveys Program. It is fully anonymized to protect respondent confidentiality, making it impossible to trace the data back to individual participants. Since our analysis uses this secondary dataset, no additional ethical approval was required for this study.

Responses