The asthma diagnosis jigsaw puzzle: an adaptable teaching concept to facilitate the diagnosis of asthma in adults and children presenting to primary care
Introduction: what is the need for improved diagnosis of asthma in primary care given the availability of national and international guidelines?
Asthma is one of the most common chronic diseases encountered in primary care. The reported prevalence of asthma varies across countries, ranging from 1%–18%1, although high rates of misdiagnosis are also well documented2,3,4. Evidence-based guidelines and consensus recommendations exist to support clinicians with asthma diagnosis5,6,7,8. For example, treatment pathways provided by the Global Initiative for Asthma (GINA), start from diagnosis based on symptoms and a demonstration of variable airflow obstruction (and/or reversibility) using peak flow and/or spirometry9. Where available, bronchodilator responsiveness (reversibility) testing is recommended for adults and children from 5 years, when they are symptomatic. However, in practice, this can be difficult as lung function is often normal when the patient is asymptomatic or has received treatment. There are currently no tests recommended for children <5 years, typically diagnosis is based on history, observation and context, often over a period of time. In this group, asthma should be suspected if there are recurring episodes of cough, breathlessness and/or wheeze occurring with or between viral infections, that respond to bronchodilators or a trial of inhaled corticosteroids, and where there is a patient or family history of atopy10.
Current guidelines and consensus statements are typically generated by respiratory specialists using data from research studies. Such guidelines are weighted towards specialist or secondary care settings and tend to be linear or algorithmic in approach. As such they do not capture or incorporate the expertise and flexibility used by expert practitioners in primary care in guideline implementation. Here, first contact presentations with multi-morbidity are increasingly common necessitating the use of multiple, sometimes overlapping, protocols, and information is often gathered in an iterative rather than linear manner11. Additionally, access to diagnostic investigations (such as routine availability of peak flow meters or spirometry) and continuity of care is either limited or absent in many countries.
Methods: how was the asthma diagnosis jigsaw puzzle teaching concept developed?
The concept of the jigsaw puzzle emerged from discussions between a small group of family physicians with an interest in respiratory care. To test and refine it as a diagnostic clinical practice and teaching concept, a multidisciplinary group of 20 primary care asthma experts from 14 countries was convened. The group included family physicians, a nurse, two pharmacists and adult and paediatric asthma specialists (Table 1). An in-person facilitated workshop was held over 2 days during the world conference of the International Primary Care Respiratory Group, followed by online consultations.
A three-round modified nominal group technique was used during the workshops12, conducted in English. This used an adapted teaching method also known as the jigsaw teaching method (Fig. 1)13 to facilitate collaboration and consensus building. Drawing on international expertise enabled content to reflect asthma diagnosis in a variety of settings, envisaging adaptation of the teaching concept across different language and resource contexts.
The asthma diagnosis, jigsaw puzzle development process.
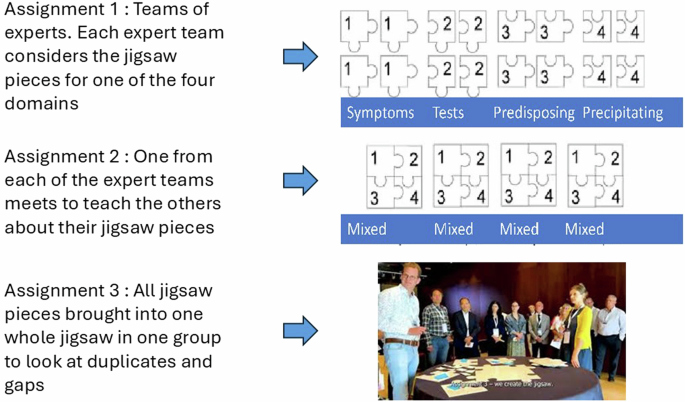
Prior to the workshop, the faculty categorised the asthma diagnostic process into four domains: presenting symptoms, physical examination and investigations, predisposing factors and precipitating factors, informed by case formulation used in biopsychosocial approaches14. Participants were advised that the goal was to build an asthma jigsaw puzzle. For Assignment 1, participants were allocated to one of the domain groups based on role, country and area of expertise. Each domain group was invited by the facilitators to discuss and agree on the most important factors—jigsaw pieces—in their domain which were described using the ‘why/how/when/who’ framework to justify inclusion (Box 1).
During the workshop, the original terms “predisposing factors” and “precipitating factors” (i.e. what prompted the presentation) were revised following vigorous debate. The final categorisation of domains was clarified as follows: Presentation, history, symptoms and physical examination and objective tests, to ease understanding of the multi-national primary care audience.
In Assignment 2, participants were each asked to move to a different table so that all four domains were represented at each table. Participants advocated for their jigsaw pieces, duplicates were prioritised and by consensus placed in the most relevant domain.
For Assignment 3, participants came together as a whole group, presenting and agreeing the final puzzle pieces required to construct a complete jigsaw puzzle. This final stage was led by two facilitators, one ensuring that all groups had the opportunity to speak, the other ensuring clarity and accuracy of language for each item of content and related descriptors.
A video summary of these stages can be seen here.
Following the in-person workshops, expert participants were invited to form a writing group. This group met three times. There was consensus that the metaphor of a jigsaw puzzle would be a helpful educational and teaching concept. The group decided that key outputs from the workshop should be a desktop helper, a practical two-page guide for global primary care and at least one peer-reviewed publication that explained the process. A sub-group finalised the desktop helper and, after trial and error, chose a famous image to illustrate the jigsaw puzzle metaphor as shown in Fig. 2.
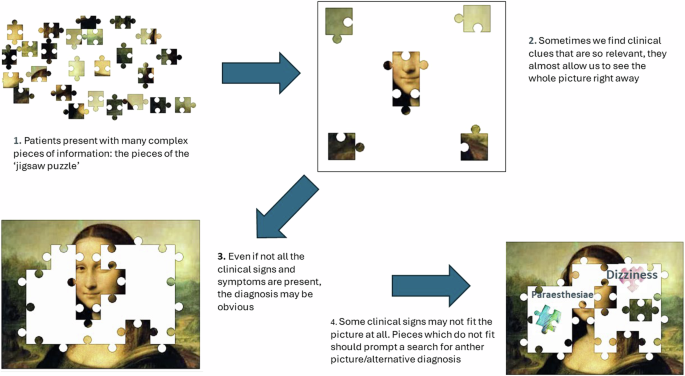
Using a jigsaw puzzle metaphor to facilitate the diagnosis of asthma in primary care.
Discussion: how does the asthma diagnosis jigsaw puzzle teaching concept add value to the challenge of asthma diagnosis?
The Asthma Diagnosis Jigsaw Puzzle is a practical and adaptable teaching concept which aims to improve confidence and competence in the diagnosis of asthma for adults and children, irrespective of resource setting. There are different ways to complete a jigsaw puzzle. A primary care clinician starts by finding the four corners, which, in the jigsaw puzzle metaphor could represent either the cardinal symptoms of asthma, (wheeze, cough, breathlessness and tight chest) or the domains (presentation, symptoms and physical examination, history and objective tests). At least some of these would point the clinician towards a diagnosis of asthma. Additional jigsaw pieces are then required to build the picture, systematically collected from the (adult) patient or, in the case of children, from the caregiver, within categories of history, physical examination and objective tests. Where puzzle pieces do not fit, they can be considered as belonging to a different picture, prompting a reformulation of diagnostic hypotheses (Fig. 2). Over time, through gathering information the picture becomes clearer, but it is only fully complete when the central pieces (in our image, the nose and mouth) are added. These are the objective test results. Where such objective tests are not available, the final puzzle picture can often still be defined, though not as clearly as when tests are utilised. It is not intended as an exhaustive list of differential diagnoses or to provide an overview of all the complexities of making a diagnosis.
The jigsaw puzzle metaphor fits intuitive, problem-solving and pattern mapping approaches mastered by expert primary care clinicians. The process of combining pieces becomes easier over time and with experience, as patterns are recognised more reliably. Just like a jigsaw puzzle, the final picture of the diagnosis gradually takes shape, as patient and clinician identify new puzzle pieces. Adaptation of the teaching concept includes both translation of key puzzle pieces across language groups, with adjustment of content to reflect commonly encountered symptoms, history, and objective tests e.g. haemoptysis – as a non-fitting piece – in settings where TB is highly prevalent.
Communication approaches using the language of puzzle completion during clinical encounters opens the possibility for patients and families to participate in the diagnostic process. Patients and caregivers are invited to gain an understanding of the complex and changing nature of symptoms and of their disease. By responding to the idea of working together with their clinician to complete ‘the puzzle’ of diagnosis, this also enables uncertainty to be visualised within the diagnostic process rather than understood as a lack of competence on the part of their healthcare provider. In some countries ‘doctor shopping’15 is common for patients in primary care, and continuity of care is particularly challenging. The value of follow up can be emphasised using a puzzle metaphor, patients and caregivers can be reassured, guided and educated by the process of working together with the clinician to achieve the diagnosis over time.
Future plans: adaptation and roll-out of teaching resources
The launch of the asthma diagnostic jigsaw puzzle teaching concept has yielded positive responses internationally, at the WONCA World 2023 Conference, the European Respiratory Society 2023 Congress, the International Primary Care Respiratory Group’s World Conference 2024, European Academy of Allergy and Clinical Immunology (EAACI) 2024 Conference and WONCA Europe conference 2024.
A new clinical practice and teaching resource, the ‘Desktop Helper no.15: the jigsaw puzzle approach to building a diagnostic picture of asthma in primary care over time’ has been translated from English and received positive feedback when used for teaching health professionals in North Macedonia. It is available online in a variety of languages (Fig. 3) and includes details of puzzle pieces in each domain which do not fit, where an alternative diagnosis may be relevant.
The asthma diagnosis jigsaw puzzle desktop helper, examples in three languages (English, Spanish, Chinese).
The development of additional resources to support teaching, learning and local adaptation of the asthma diagnosis jigsaw puzzle teaching concept is underway. These include locally developed case vignettes. The fidelity of the jigsaw puzzle metaphor as an adaptable teaching concept will be tested through evaluation of upcoming workshops in Uganda, Malaysia and India.
Conclusion
The variability of asthma symptoms over time and the absence of any single objective diagnostic test poses a problem for diagnosis of asthma internationally. Achieving the correct diagnosis is essential to ensure adults and children receive the right care including pharmacological treatment with inhaled medications and non-pharmacological interventions. The asthma diagnosis jigsaw puzzle teaching concept is a succinct, adaptable symptom-based approach relevant for first contact and follow-up clinical encounters in primary care. It has the potential to support more effective diagnosis of asthma and improved clinical outcomes, along with the delivery of patient-centred care. Teaching resources have been developed and are being disseminated internationally.
Responses