To choose or not to choose? A study on decision-making for virtual reality intervention in children with ADHD
Introduction
Attention Deficit Hyperactivity Disorder (ADHD), also known as hyperactivity disorder (Xin 1994), is a neurodevelopmental disorder. ADHD is often accompanied by symptoms of inattention, poor self-control and impulsivity and is a risk factor for a range of other mental health problems (Sayal et al. 2018), with serious implications for children’s academic performance, social interactions, personality and character development (Peasgood et al. 2016). ADHD affects approximately 5–10% of children worldwide. According to epidemiological survey data on mental disorders in Chinese children and adolescents in 2021, there are up to 23 million children with ADHD in China alone (Peng, 2021). Consequently, effective intervention and treatment for ADHD have been focal points of clinical and academic research.
Currently, the main treatment for ADHD is to alleviate the core symptoms through medication, but the long-term effect of this treatment is not ideal (Xin 1994), and there are certain side effects (O’Leary 1980). Due to the influence of children’s family, social and personal factors, adherence to medication is difficult to ensure in practice, and medication adherence is poor in paediatric patients (Wang et al. 2020). In recent years, safe and effective non-pharmacological interventions have become a trend in the treatment of ADHD, with Virtual Reality (VR) technology becoming a new frontier in this domain (Hollis et al. 2017; Torous et al. 2021). This intervention programme has the potential to enhance children’s concentration, social skills, and self-control by generating targeted virtual environments. However, the efficacy, feasibility, and adaptability of VR intervention require validation by long-term research data. Would Chinese parents be willing to select VR-based intervention programmes for their ADHD-afflicted children given the potential risks associated with this burgeoning technology? What are the key considerations that inform their decision-making process? The theory divides the risk decision-making process into two phases, editing and evaluation, characterised by a value function and a weight function; the editing phase carries out the collection and recombination of data, and the evaluation phase generates a value function and a weight function based on the information from the previous phase, leading to the completion of the decision. We constructed a binary logit regression model with four dimensions of preference structure, belief characteristics, community participation and decision readiness and 23 explanatory variables. The first three dimensions are the influences on the generation of value function and weight function in the decision formation process under prospect theory. Through the analyses, this study investigated the decision-making process of parents of children with ADHD in choosing a virtual reality intervention programme and explored their psychological preferences and influencing factors in the decision-making process.
Research review
An evolving theoretical framework for behavioural decision making in healthcare choices
The behavioural decision-making in medical choices primarily investigates the decision-making process and behavioural patterns individuals exhibit when confronted with medical choices. Treatment choice is a multifaceted research subject, encompassing decisions made by individuals based on their needs, expectations, environmental resources, and external constraints (Shi 2021). In the early 1960s, scholars began to focus on medical decision-making theories (Zhang et al. 2012). Subsequent empirical studies explored the factors affecting patients’ medical behaviours, including the quality of clinical communication between parents and physicians (Salmon and Young 2013), parents’ familiarity with medical knowledge (Li et al. 2022), the content of information accessed on social media (Xu and Ma 2018; Yang and Chao 2021), the level of support provided by online communities (Sun and Kang 2022), urban-rural or cultural disparities (Brown et al. 2015; Chen et al. 2019), and household income (Abera et al. 2015), among others. These empirical investigations into patient behavioural decision-making have extended from a medical perspective to sociological, economical, psychological, and communicational domains. With the continuous evolution of research, scholars are endeavouring to devise theoretical tools that accurately depict patient decision-making(Li and Song 2010). the Andersen Model predicts medical choice outcomes from a demand and supply perspective (Andersen and Kravits 1976); the Expected Utility Theory posits that individuals’ decision-making will opt for the option with the maximum expected utility; the Mental Accounting Theory proposes that individuals categorize and evaluate economic or psychological costs and benefits in decision-making, and make decisions based on the balance of different accounts. Currently, the field of behavioural decision-making in healthcare choices faces methodological challenges, such as how to accurately collect and process data in empirical studies to measure individual preferences, emotions and cognitive processes. How to explore VR intervention choice decisions for children with ADHD based on empirical methods remains an area to be explored. This study used Prospect Theory (PT) as a theoretical framework for behavioural decision-making, which suggests that individuals’ attitudes towards risk and uncertainty in healthcare choices may not only be based on expected utility, but also be influenced by their perceptions of losses and gains. The inherent consistency of Prospect Theory with decision-making under conditions of risk makes it applicable to understanding healthcare choices.
Decision-making for VR interventions based on prospect theory
Prospect Theory, introduced by Daniel and Amos in 1979, is a behavioural economic theory designed to elucidate decision-making processes and individual characteristics under risk conditions. It posits that individuals are not entirely rational in their attitudes towards risks and rewards. Specifically, when faced with potential gains, individuals prefer certainty to risk; when faced with potential losses, people are more inclined to take a’gamble’.
In the information editing stage, parents gather information related to virtual reality from various sources; they then combine this information with their own preference structures, belief traits, and situational factors to form decisions. There are three main types of situations that influence their personal preferences: 1. Representativeness heuristic: the treatment choices and outcomes of ADHD families in the online community influence other families’ assessment of treatment options. 2. Availability heuristic: refers to the ease with which patients and their parents can access detailed information about treatments – including media reviews, advertisements released and treatment behaviours provided by physicians’ degree of guidance – the ease with which they can do so. 3. Anchoring and adjustment: a theory in psychology that measures behavioural decision-making. Factors affecting anchoring values may include the child’s condition, the parents’ mental calculations of the cost of treatment, and expectations of outcomes (Kahneman and Tversky 1979).
The time and transport costs of VRT were also key factors influencing the preference structure during the assessment phase. Parents compare the prospect of virtual reality therapy constructed in the previous phase with other methods and weigh them to make a final decision based on their mental readiness, which corresponds to the weighting function in prospect theory.
Based on the theory and logical derivation, we propose three stages of the parental decision-making process. In the first stage, by compiling information about the treatment plan to form a belief profile, parents determine the expected value of their child’s health stock based on their own beliefs and preference structure; by ‘simplifying and synthesising’ the expected value and its influencing factors, they are prepared for subsequent risk assessment and decision-making choices. In the second stage, the patient’s preference structure is assessed, the parents calculate the expected value of the virtual reality (VR) intervention technology, and the information collected in the editing stage is measured to generate a value function and a weighting function. The third stage is then the patient’s healthcare behavioural decision, where the parents decide whether to choose the virtual reality intervention technology for their child (Fig. 1).
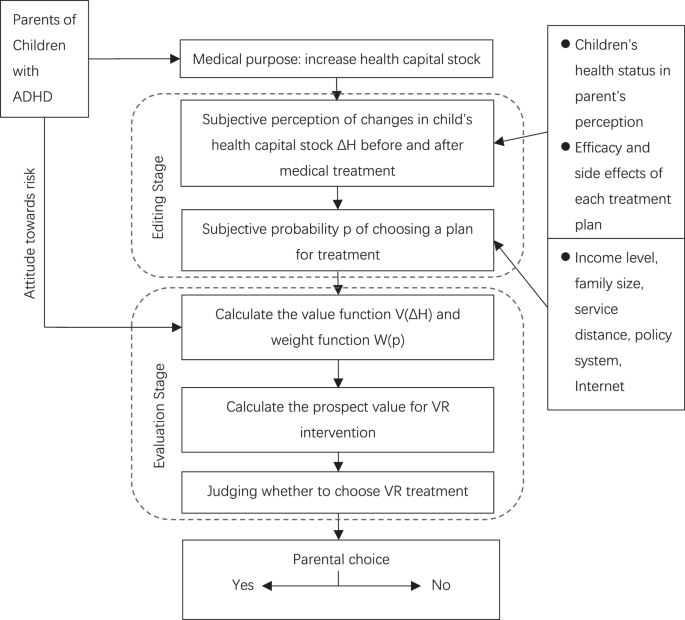
Including two stages, upper dotted box shows the editing stage, where different “prospects” (child’s health capital stock, effects of each treatment, etc.) are simplified and recoded. Lower dotted box shows the evaluation phase, where the edited prospects are evaluated and the highest-value choice is ultimately made.
The use of virtual reality in the treatment of ADHD in children
Studies have shown that medication, the first treatment option considered, is not ideal in practice due to children’s family and personal factors, such as on-time and adherence to medication (Wang et al. 2020). At the same time the focus on children with ADHD in the fields of behavioural, neuroimaging and genetic sciences has provided new perspectives and stimulated new therapeutic approaches to our understanding of the underlying pathophysiological mechanisms of ADHD (Shaw et al. 2014). Virtual reality intervention techniques, as an emerging therapeutic approach, offer some advantages over traditional pharmacological treatments (Bashiri et al. 2017).
Virtual Reality (VR) technology replaces user perception in the real world by digitally generating perceptual experiences. It has the advantages of being immersive, easy to operate, not limited by time and space, and accurately simulating real-world scenarios. In the field of behavioural interventions, VR technology has been combined with classroom tasks (Bioulac et al. 2020), serious games (Rodrigo-Yanguas et al. 2021), physical training (Shema-Shiratzky et al. 2019), and neurobiofeedback training (Oh et al. 2022), proving its effectiveness in reducing the attention shifting frequency and enhance patients’ cognitive abilities and executive function.
By creating a precisely controlled virtual world for the user, virtual reality technology facilitates therapeutic interventions (Freeman et al. 2017; Hatta et al. 2022b, 2022a). Numerous studies have confirmed the ability of VR technology to create virtual environments for diagnosis, training, monitoring, assessment and treatment to provide optimal rehabilitation for children with ADHD (Bashiri et al. 2017; Romero-Ayuso et al. 2021). Studies have identified key advantages of virtual reality as a treatment modality for ADHD: (1) providing a safe and controlled environment for children to practice and develop cognitive skills such as attention and impulse control; (2) enabling children to manage distractions and improve attention by immersing them in a virtual environment; (3) providing a non-pharmacological alternative for children with ADHD who are intolerant or unresponsive to medication; (4) serve as a valid assessment tool to better evaluate ADHD symptoms and improve diagnostic accuracy; and (5) demonstrate effective outcomes in terms of enhanced sustained attention, measures of alertness, increased number of correct responses, and reduced number of errors of omission (Schweitzer and Rizzo 2022). Despite the encouraging short-term results of VR interventions for ADHD, the effectiveness, feasibility, and adaptability of VR as a treatment modality need to be validated through long-term research data. Currently, there is a lack of clinical trial data to support its long-term effects and potential side effects; the requirement for specialised equipment and technical support results in high costs; and some children have shown adverse reactions to VR technology, experiencing symptoms such as dizziness and headaches during assessment or training.
In summary, this study identifies the factors that influence parents’ willingness to choose a virtual reality intervention programme for their children based on a prospective theoretical framework and classifies them into three categories: 1. Preference structure, which includes the price and time costs parents are willing to pay, and demographic and individual characteristics of parents; 2. Belief characteristics, encompassing media reviews, advertisement releases, the extent of treatment behaviour guidance provided by doctors, the child’s condition, parents’ psychological calculations of treatment costs, and their expectations of treatment outcomes; 3. Online community involvement, referring to the information parents acquire through participation in online communities.
Based on the above, we propose the following hypotheses:
H1: Preference structure influences parents’ decision readiness.
H2: Belief characteristics influence parents’ decision readiness.
H3: Online community involvement affects parents’ decision readiness.
H4: Parents’ decision readiness ultimately leads to their decision.
Using the research hypotheses and variable settings, we establish a structural equation model to describe the decision-making path and outcomes of patient medical behaviour. The model comprises four latent variables: belief characteristics, preference structure, community involvement, and decision readiness. From a relationship perspective, belief characteristics, preference structure, and community involvement influence decision readiness, which in turn affects the final decision outcome (Fig. 2).
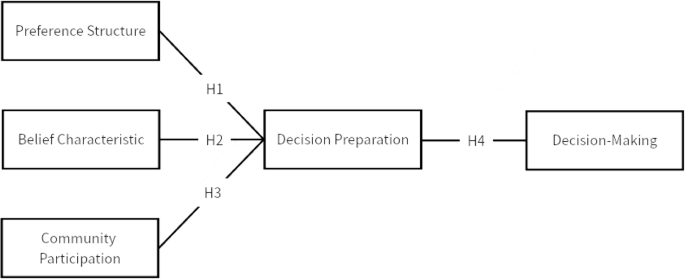
A structural equation model includes variables of belief characteristics, preference structure, community involvement that influence decision preparation, ultimately affect decision making.
Research design
Methodology
Grounded in Prospect Theory (PT) and drawing from paradigms in behavioural economics and cognitive psychology, this study aims to elucidate the factors influencing parents’ willingness to choose treatment modalities for their ADHD-affected children. The dependent variable is the parents’ intention to select a treatment, while the independent variables encompass 23 factors across four dimensions: preference structure for VR-based interventions, belief characteristics, participation in online communities, and decision readiness. These factors include understanding of VR therapy, trust level, information acquisition channels, time costs, and price costs, among others. A binary Logit regression model was constructed based on a quantitative survey to analyze the determinants of parents’ treatment choices.
The introductory section of the questionnaire provides an objective and detailed overview of the ADHD treatment options currently available in China. This predetermined information informs parents about possible ADHD treatments and their impact on their child’s health. The questionnaire items were developed and refined based on existing research. The preference structure section was developed referencing the study by Haiming Liang et al. (2018). The belief characteristics section drew from the works of Tao Jiang (2013) and Wiebe Annika et al (2022). Specific questions for each dimension are presented in Table 1. Respondents were asked to indicate their level of agreement using a Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree), with X24 requiring a binary choice. Prior to the main survey, a pilot study involving 50 participants was conducted to validate the reliability, validity, and correlation of the self-developed questionnaire. The results affirmed the instrument’s reliability and validity. (Table 1).
Data collection
The link of the questionnaire generated through the “Wenjuanxing” website (https://www.wjx.cn) was distributed to several online groups of parents of children with ADHD. A total of 477 questionnaires returned and 413 deemed valid, resulting in an 86.6% validity rate. Demographic details of the 477 respondents are presented in Table 2.
Results
Measurement model
The reliability, validity, and correlation of the self-developed questionnaire were assessed. The Cronbach α coefficient stood at 0.859, surpassing the 0.8 threshold. The Kaiser-Meyer-Olkin (KMO) value was 0.910, indicating satisfactory sampling adequacy. Exploratory factor analysis revealed that items X8 and X10-15 had low correlations with the questionnaire, making it challenging to ascertain their influence on parents’ treatment decisions. Consequently, these items were excluded prior to the main survey. The remaining items exhibited communalities above 0.4, suggesting strong correlations between the research items and the underlying factors.
Structural equation modelling (SEM)
SEM, a multivariate data analysis technique, was employed to examine the relationships between multiple latent variables. To evaluate the model’s fit, fit indices such as the χ²/df ratio, Root Mean Square Error of Approximation (RMSEA), and Goodness of Fit Index (GFI) were considered. The χ²/df ratio was 2.951, GFI was 0.912, and RMSEA was 0.069, indicating a high model fit. Furthermore, standardized regression coefficients for most factors and items exceeded 0.5, signifying significant relationships with item 25 (Table 3).
The SEM results model and data are shown in the Fig. 3 below:
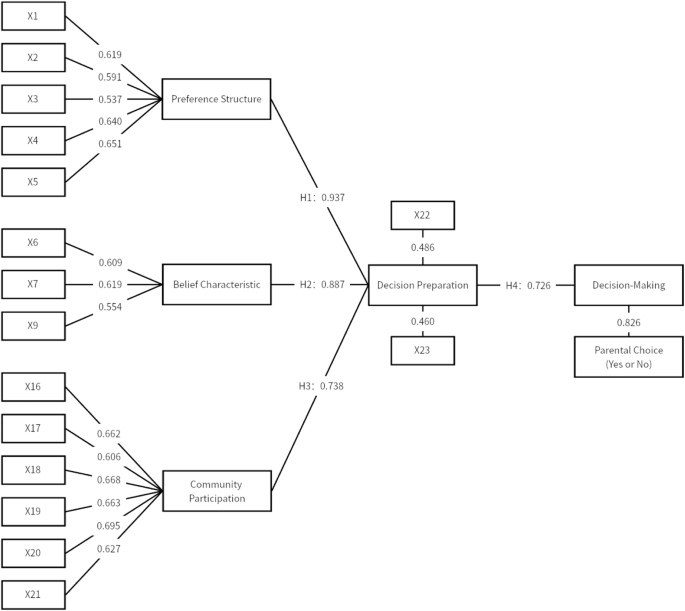
SEM results model.
Binary logit analysis
Following confirmatory factor analysis and SEM validation, the influence of each survey item on parents’ decision outcomes was further explored using binary Logit analysis. Out of the 413 valid samples, 363 parents chose “yes” (indicating a preference for VR intervention), while 50 opted for “no.” These responses were coded as “1” for “yes” and “0” for “no.” The final binary Logit regression model yielded a chi-square value of 160.176 with a p value of 0.000, confirming the model’s validity. The results of the regression analysis for each question are shown in Table 4.
Regression results revealed that items X2, X3, X9, X17, and X21 significantly influenced parents’ decisions.
Binary probit analysis
To validate the findings from the binary Logit analysis, the survey was subjected to a binary Probit analysis, a similar analytical tool. The results from the Probit analysis aligned with those from the Logit analysis, as depicted in Table 5.
Discussion
From the statistical results presented in the table above, it is evident that the preference structures of parents, their belief characteristics, and participation in online communities have a statistically significant influence on their final decision-making. Through binary Logit and Probit analyses, it is discerned that questions within the preference structure category (X2: “I believe virtual reality technology can effectively alleviate symptoms of ADHD in children”; X3: “I am aware of the pros and cons of virtual reality therapy”) and belief characteristics category (X9: “I have the patience and energy to ensure my child continues with virtual reality therapy”) as well as those within the online community participation (X17: “I frequently post in online communities related to children with ADHD”; X21: “I believe online communities offer better treatment information than other websites”) play pivotal roles in parents’ decisions regarding VR intervention programmes. The individual preference structures, belief characteristics, and online community participation of parents can lead to irrational behaviours and frame-dependent effects, thereby influencing their decision-making.
Many medical studies have revealed the underlying pathomechanisms of ADHD and summarised various treatments, the most prominent of which currently remains pharmacological treatment (Liu and Zhong 2019). Available medications include stimulants (methylphenidate, amphetamine) and non-stimulants (atomoxetine, guanfacine, colistin); although pharmacological treatment regimens for ADHD have shown better treatment outcomes and overall good drug tolerance in short-term trials, there is still a need for improvement of current treatment strategies and development of novel drugs (Mechler et al. 2022).
At the present stage, there has been a significant shift in parents’ preferences for intervention methods for children with ADHD. They have shown a strong interest in emerging technologies, particularly high-tech interventions like VR, which they trust and find more appealing. After carefully considering its pros and cons, parents acknowledge the benefits that VR offers. During the information editing phase, parents considering VR as an intervention for their children would assess the health gains or losses quantitatively, in line with Prospect Theory. Parents typically use the benefits derived from traditional treatments as a benchmark for the child’s existing health status. They believe that high-tech treatments such as Virtual Reality (VR) augment therapeutic outcomes for children with ADHD, offering greater anticipated benefits than conventional drug and physical therapies. Moreover, parents discern the probable harmful effects of VR interventions as compared to traditional interventions, choosing the one with fewer drawbacks. They consider the possible adverse consequences of VR interventions on children to be more tolerable than the adverse reactions of other treatment methods.
In families with children diagnosed with ADHD, parents prioritize providing the best possible treatment for their child, even if there are financial and time costs to consider. This emphasizes the importance of children’s health to modern parents, who prioritize it over economic and temporal concerns when choosing a treatment plan. This decision-making behaviour lacks the basis of rational agent decision-making, which involves using the Expected Utility Theory and opting for maximum utility. Instead, it stems from a psychology that involves risk-taking, leading to decisions based on relativity instead of absoluteness. This phenomenon aligns with the Prospect Theory, which underscores high costs for children’s health. As previous research has suggested, with the advancement of shared decision-making models, parents now place greater value on and anticipate participating in medical decisions regarding their children’s healthcare. This often results in higher health expectations, with economic costs taking a back seat. Specifically, parents express greater willingness to invest in high-tech treatment options (Tuman and Ivankovich 1993).
When selecting virtual reality technology as an intervention for their child’s ADHD, parents often turn to online communities for advice and recommendations to aid in their final decision-making. In the past, parents solely relied on doctors for treatment plans, which was due to inducements from medical market providers and information asymmetry between doctors and patients (Banerjee 1992; Raafat et al. 2009). With the increasing prevalence of online communities, parents are more frequently involved in community discussions to decide on treatment plans for children with ADHD. Online forums have become their primary medium for decision-making, surpassing national platforms, television, hospital promotions, and other traditional media sources (Sun and Kang 2022). This shift away from conventional media towards social media aligns with contemporary changes in media and trust. The public’s trust in emerging media has transitioned from traditional official sources due to the shift in the mass media trend towards smaller community sources. These days, people increasingly turn to new media to seek medical consultations, treatment plans, and news, just as parents do when making healthcare decisions for their children.
In conclusion, VR Digital Health Interventions (DHI) represent a significant trend in future medical advancements amidst the evolution of the metaverse. This study suggests that parents’ decision-making in choosing such interventions for their children is a complex behavioural process that generally reflects acceptance of new technology. This acceptance requires weighing both advantages and disadvantages carefully. However, this balancing activity is not based on rational decision-making by agents but is rooted in a psychology of risk-taking. Decisions are made based on relativity rather than absoluteness. Additionally, online community information easily influences decisions, leading to deviations from benefit maximization. Children’s health is prioritized over economic and time costs.
Limitations
This study focused on whether parents would choose VR as an intervention for their child’s ADHD and did not examine the psychological decision-making of parents when faced with all available treatment options. Therefore, the results of data analysis should not be used as a separate reference for medical decision-making.
Parents’ decision-making in choosing disease interventions for their children is a complex behavioural process. Future research aims to further explore the decision-making process of parents when selecting different treatment options for children with ADHD. A more diversified research methodology, such as combining the conduct of in-depth interviews, will be used to examine additional factors that impact parents’ choices of intervention methods. These findings will contribute to more comprehensive recommendations for medical institutions and parents seeking intervention methods for children with ADHD.
Responses